





Volume 215 - Issue 2
Are COVID‐19‐safe Tokyo Olympics and Paralympics really possible?
Authors: Craig B Dalton and Joanne Taylor
Med J Aust 2021; 215 (2): 54-55.e1. || doi: 10.5694/mja2.51159
Published online: 19 July 2021
Published online: 19 July 2021
The Olympic Games raise many infection control, health security and ethical challenges
The Olympic Games raise many infection control, health security and ethical challenges
Signs in the windows of Tokyo’s Tachikawa Sogo Hospital declare “Medical capacity has reached its limits. Stop the Olympics!” Another asks, “Give us a break”. Support for the Olympic Games is dwindling; as is confidence in a coronavirus disease 2019 (COVID‐19)‐safe event in the midst of Japan’s uncontrolled community transmission of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). While the Tokyo Olympics and Paralympics provide athletes with opportunities to compete on the world stage, and international viewers with a much‐needed break from pandemic news, the decision by the International Olympic Committee (IOC) and Japan to forge ahead with such a large scale, international event raises many infection control, health security and ethical challenges.
Let’s first acknowledge some of the steps being taken by the IOC to limit COVID‐19 transmission. The absence of international spectators, decreasing crowding in the Olympic Village, standard physical distancing, pre‐departure and daily testing of athletes, and limiting athletes’ arrivals to 5 days before, and departure within 48 hours of, competition will all provide some protection.1 While the IOC encourages vaccination and has signed a memorandum of understanding with Pfizer–BioNTech to provide free vaccination for Olympic athletes, it is not mandatory for attendance.1
However, these interventions are likely to be inadequate. From a governance perspective, we cannot expect a country with thousands of cases per day to deliver a COVID‐19‐safe Olympics in mid‐July. As opposed to Australia’s COVID‐19 suppression strategy, throughout the pandemic, the Japanese government has taken a cluster‐based approach to the COVID‐19 response, characterised by targeted response to identified clusters of more than five cases alongside broad acceptance of the inevitability of community transmission of SARS‐CoV‐2.2
The first point of concern is that Japan is in its fourth COVID‐19 wave and third state of emergency, with over 3000 cases being reported daily in early June — and this is likely to be an underestimate of the true case count (Box). Despite Japan having had at least five times the number of cases per head of population from the beginning of the pandemic until the end of May, it has only conducted 11 900 000 tests in a population of 126 million compared with 17 295 000 tests in a population of 26 million in Australia.3 Acknowledging some of these are repeat tests, these statistics approximate one test for every 1.5 people in Australia compared with one test for every 11 people in Japan. Reasons for reduced testing capacity include the lack of investment in expanding testing and digitalisation in the health care system,4 with Japan likely missing COVID‐19 cases because of testing limitations. In addition, to early June, only 7% of the population has been fully vaccinated.5
Second, there is the risk to people participating in the Games. While the Olympic Village is intended to be a bubble with limited contact with the Japanese population, there will be inevitable contact between service providers for cleaning, transport, COVID‐19 testing, security and catering. As seen in Australia, such bubbles are vulnerable to leaks of SARS‐CoV‐2 despite stringent infection control practices. Furthermore, as early as April, 40% of infections detected in Tokyo were attributed to a variant of concern, posing additional risk to participants and their home country via ongoing transmission after the Games.6
The proposed pre‐arrival testing plan, critical to preventing the introduction of SARS‐CoV‐2 strains into the Olympic Village, is questionable. The IOC is requiring Games attendees to have two negative COVID‐19 tests in the 96 hours before arrival in Tokyo.1 Unfortunately, rapid antigen tests, which are much less sensitive than polymerase chain reaction (PCR) tests, are the only tests available for many athletes from limited‐resource settings where COVID‐19 is raging. The official certificate of testing for COVID‐19 is a manually completed form downloaded from the internet.7 While the form needs to be signed by a doctor and should include the name and address of the laboratory, the name of the signing doctor is not required. The form must have an “imprint of a seal”, but evidence of participation in a modern laboratory quality assurance program is not required.
The proposed athlete testing strategies may not be feasible. While athletes will undergo daily COVID‐19 salivary testing (rapid antigen‐based, with PCR confirmation of positive rapid tests), it is proposed that all 11 000 athletes will gather daily at a dedicated testing area in the Village to ensure testing.1 The logistics of this testing regimen, which is more than the typical daily test peak of 10 000 people in the entirety of Tokyo,3 and the opportunity for transmission within this single location must be considerable.
Then there is the risk presented by congregate living within the Olympic Village. COVID‐19 outbreaks in nursing homes, cruise ships and homeless shelters demonstrate that congregate settings amplify SARS‐CoV‐2 transmission.8,9,10 The main accommodation is comprised of multiple 14–18‐storey apartment buildings with internal shared hallways and lifts. Apartments will be shared and the Japanese summer will discourage the use of natural ventilation. We have learned from quarantine hotel transmission incidents that completely COVID‐19‐safe accommodation may need to be purposely built to control aerosol transmission. The proposed infection control interventions may ameliorate transmission, but mass gatherings such as the Olympic Games have a long record of outbreaks due to multiple shared indoor spaces.11,12 Many of the proposed infection control protocols in The Playbook: athletes and officials — your guide to a safe and successful Games, published in April 2021 by the IOC and local Japanese organisers, appear half‐hearted by Australian standards.1 For instance, the Playbook states that “seating capacity will be limited to allow for physical distancing — for example, a table for six will be adjusted to seat four people”. According to the Playbook, close contacts (ie, ≥ 15 minutes within one metre) of confirmed cases of COVID‐19 may not be subject to compulsory 14‐day quarantine, as practised in Australia. They may be allowed to compete if symptom and laboratory testing criteria are met. Games attendees are required to download the Japanese Contact Confirming Application (COCOA) smartphone application (app) — the equivalent of the COVIDSafe app in Australia — which is due for release in June, allowing only weeks of real‐world trialling before its implementation for the Games. This may be a revised version of the current COCOA app, which appears beset with problems similar to the Australian COVIDSafe app.13
On the ethical challenges for Australia, there is no doubt that Australian athletes, coaches, doctors and support staff travelling to a country at high risk of COVID‐19 transmission to represent their country deserve to be protected with a COVID‐19 vaccine. Upon return to Australia, unless alternative infrastructure is developed, the approximate 1000 Games attendees will then require quarantine hotel space that could be used to reunite long separated families. Consideration must also be given to what happens if issues relating to variants of concern arise in Japan, similar to what happened in India. Will the Games attendees be in a similar position to the cricketers? Will sick Olympians and Paralympians be able to access care in an overwhelmed health system?
The Games raise ethical concerns for Japan as well. Sixty per cent of Japanese citizens surveyed wanted the Olympics cancelled amidst a growing online protest campaign.14,15 Many recognise the potential impacts on Japan of the arrival of a large contingent of travellers from countries ravaged by variants of concern.
Japan and Australia can make a risk–benefit analysis of conducting or participating in the Games. There are obviously many dreams and careers hanging in the balance and it would be a dour world if all risky human activities had to be blessed by public health practitioners. Throughout the history of plagues and pandemics, people have sought a rapid return to normality at the first opportunity. But claims of a guaranteed COVID‐19‐safe Olympics at this time are at best an aspirational goal and at worst a cynical public relations platform. The IOC’s dogged insistence — regardless of external realities — that the Games will go ahead should be concerning. There should have been a nuanced acknowledgement of the factors that would trigger the cancellation of the Games and, at the minimum, a thorough review of risk mitigation strategies during the planning phase.16 Global surveillance for COVID‐19 among Olympics returnees, and locally in Japan, can inform mass gathering risk assessments during the next phase of the pandemic.
Box – Daily new coronavirus disease 2019 (COVID‐19) cases in Japan from 3 January 2020 to 3 June 2021
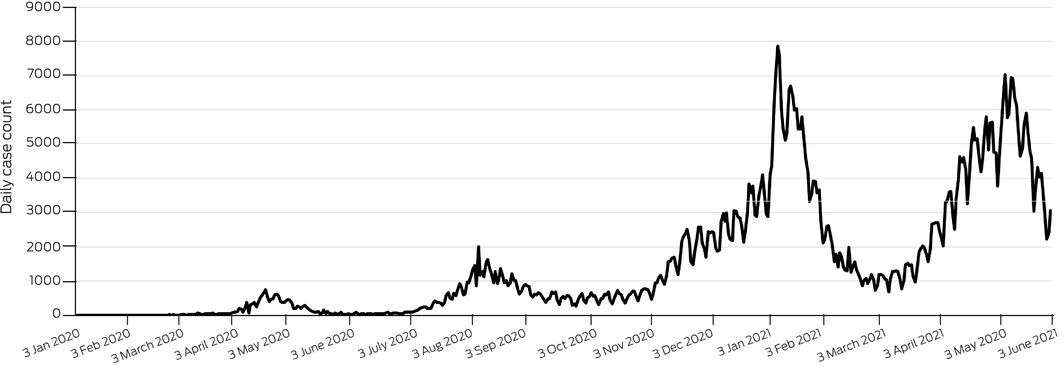
There have been 752 191 COVID‐19 cases diagnosed in Japan, with four evident waves of increased transmission occurring during April–May 2020, August–September 2020, January–February 2021 and April–present 2021.
Competing interests
No relevant disclosures.
Acknowledgements
We would like to acknowledge Stephanie Wheeler for review and suggestions to improve the manuscript.
References
- International Olympic Committee; International Paralympic Committee. The Playbook: athletes and officials — your guide to a safe and successful Games (April 2021, version 2). Tokyo: IOC, 2021. https://stillmed.olympics.com/media/Document%20Library/IOC/Olympic-Games/Tokyo-2020/Playbooks/The-Playbook-Athletes-and-Officials-April-2021.pdf?_ga=2.160631161.516743386.1620880077-509195702.1620880077 (viewed May 2021).
- Shimizu K, Tokuda Y, Shibuya K. Japan should aim to eliminate COVID‐19. BMJ 2021; 372: n294.
- Tokyo Keizai. Coronavirus disease (COVID‐19) situation report in Japan. https://toyokeizai.net/sp/visual/tko/covid19/en.html (viewed June 2021).
- Shimizu K, Wharton G, Sakamoto H, Mossialos E. Resurgence of COVID‐19 in Japan. BMJ 2020; 370: m3221.
- Reuters Vaccine Tracker. Japan. https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/japan/ (viewed May 2021).
- Current Situation of Infection, April 27, 2021 National Institute of Infectious Diseases, Japan. Available at: https://www.niid.go.jp/niid/en/2019-ncov-e.html (viewed May 2021).
- Ministry of Health, Labour and Welfare, Japanese Government. Certificate of testing for COVID‐19. https://www.mofa.go.jp/files/100177968.pdf (viewed May 2021).
- Arons MM, Hatfield KM, Reddy SC, et al. Presymptomatic SARS‐CoV‐2 infections and transmission in a skilled nursing facility. N Engl J Med 2020; 382: 2081–2090.
- Expert Taskforce for the COVID‐19 Cruise Ship Outbreak. Epidemiology of COVID‐19 Outbreak on Cruise Ship Quarantined at Yokohama, Japan, February 2020. Emerg Infect Dis 2020; 26: 2591.
- Tobolowsky FA, Gonzales E, Self JL, et al. COVID‐19 outbreak among three affiliated homeless service sites — King County, Washington, 2020. MMWR Morb Mortal Wkly Rep 2020; 69: 523–526.
- Hoang VT, Al‐Tawfiq JA, Gautret P. The Tokyo Olympic Games and the risk of COVID‐19. Curr Trop Med Rep 2020; 30: 1–7.
- Stuart M, Kwon YI, Rhie SJ. Pharmacy services at the PyeongChang 2018 Olympic and Paralympic Winter Games. Br J Sports Med 2019; 53: 1105–1110.
- Limited testing leaves COVID‐19 app glitches overlooked. The Japan Times 2021; 16 Apr. https://www.japantimes.co.jp/news/2021/04/16/national/virus-app-glitches/ (viewed June 2021).
- Change.org. Cancel the Tokyo Olympics to protect our lives. https://www.change.org/p/cancel-the-tokyo-olympics-to-protect-our-lives-stoptokyoolympic-cancelthetokyoolympics (viewed June 2021).
- Lies E, Kihara L. Amid opposition, Japan PM says has “never put Olympics first”. Reuters 2021; 10 May. https://www.reuters.com/world/asia-pacific/poll-shows-60-japanese-want-games-cancelled-2021-05-10/ (viewed June 2021).
- Sparrow AK, Brosseau LM, Harrison RJ, Osterholm MT. Protecting Olympic participants from COVID‐19 — the urgent need for a risk‐management approach. N Engl J Med 2021; https://doi.org/10.1056/NEJMp2108567 [Epub ahead of print].
Provenance: Not commissioned; externally peer reviewed.