




The known: The prevalence of inflammatory bowel disease (IBD) is increasing worldwide. However, recent age‐standardised prevalence data for Australia are not available.
The new: The age‐standardised IBD prevalence rate of 348 cases per 100 000 population we found is the highest ever reported in Australia. Its prevalence was higher in older people: 612 per 100 000 people aged 65 years or more and 891 per 100 000 people aged 85 years or more.
The implications: Given the higher prevalence of IBD among older people in metropolitan Sydney, and their higher risk of infections, doctors should consider replacing systemic immunosuppressive therapies with alternatives when possible.
The worldwide burden of inflammatory bowel disease (IBD), which includes Crohn disease and ulcerative colitis, has increased markedly over the past sixty years,1 partly because IBD is incurable but rarely fatal.2 Its prevalence is greatest (but stable) in western Europe and North America,1 but its incidence has risen over the past two decades in more recently industrialised countries in Asia, South America, and Africa.3,4
The burden associated with IBD in Australia is high; it was estimated to have incurred more than $2.7 billion in costs in 2012.5,6 Earlier epidemiological studies in Victoria (2010–11)5 and Tasmania (2013–14)7 included mixed urban and rural populations; in a multi‐nation Asia–Pacific study, epidemiological variations were associated with population density and proximity to metropolitan areas.8 Young people with IBD may move to cities for education and employment, reducing the apparent prevalence of IBD in rural areas.
It was recently reported that IBD prevalence rates in Lothian (Scotland) were very high among people aged 60–79 years (1178 per 100 000) or 80 years or more (1042 per 100 000), and they are projected to rise further by 2028.9 The use of immunosuppressive therapies to treat IBD in these age groups is problematic, as opportunistic infections, sepsis, comorbid conditions, and malignancy are more frequent in older patients.
We therefore examined age‐specific prevalence rates of IBD in a defined metropolitan area of Australia, focusing on its prevalence in older people.
Methods
Population characteristics
We assessed the prevalence of IBD in the City of Canada Bay, a local government area in the inner west of Sydney, with a population of 88 015 at the time of data collection (Box 1).10 Concord Hospital, a centrally located public hospital with an established IBD clinic, provides free health care for patients with IBD.
Data collection
We analysed clinical data for people with IBD living in the City of Canada Bay (postcodes 2046, 2047, 2137, 2138) during 1 March 2016 – 10 November 2016, including those reviewed by gastroenterologists outside the study area. We identified people treated at Concord Hospital according to International Classification of Diseases, 10th revision (ICD‐10) coding. We also obtained information on patients from gastroenterologists and colorectal surgeons at Concord Hospital, private gastroenterology and colorectal surgery practices, the Sydney IBD database (ambulatory IBD patients identified in medical records from Concord Hospital and City of Canada Bay community gastroenterologists), and the paediatric IBD database of the Westmead Children’s Hospital.
Two authors (AP, JL) collected patient data in standardised forms. Given the heterogeneity of the data sources, various search methods were employed to identify patients, including searches for keywords (eg, Crohn, colitis, IBD), pharmaceutical prescriptions, and ICD‐10 codes. Demographic data (patient’s initials, sex, age, postcode) were collected to check for duplication and for analyses of point prevalence. “Older person” was defined as someone aged 65 years or more. Clinical data (IBD subtype, age at diagnosis) were obtained from patient medical records. The most recently updated IBD phenotype details (according to the Montreal classification11) were also collected.
Inflammatory bowel disease: diagnostic criteria
We included only patients with confirmed IBD according to the internationally recognised Copenhagen12,13 (Supporting Information, table 1) and revised Porto criteria14 for clinical, endoscopic, radiological and histological findings. Each included IBD case was independently verified by two of the authors (AP, JL).
Data analysis
Crude IBD prevalence rates were calculated by dividing the number of confirmed cases by the City of Canada Bay resident population; rates were separately calculated for Crohn disease, ulcerative colitis, and IBD unclassified (IBDU). Rates, with 95% confidence intervals (CIs), were expressed per 100 000 population. Direct age standardisation was based on the World Health Organization standard population,15 permitting comparisons with overseas data; 95% CIs were calculated with the Keyfitz formula.16 Statistical analysis was performed in the Statistical Package for the Social Sciences (SPSS) Statistics 23.
Ethics approval
Our study was approved by the Sydney Local Health District Human Research Ethics Committee (reference, HREC/16/CRGH/21).
Results
Demographic characteristics and phenotypes
We identified 364 prevalent cases of IBD; the median age of patients was 47 years (interquartile range [IQR], 34–62 years; range, 7–100 years), and 185 patients were women (50.8%). The median duration of IBD was 8 years for Crohn disease (IQR, 4–17 years), 10 years for ulcerative colitis (IQR, 4–18 years) and 11 years for IBDU (IQR, 4–14.5 years) (Box 2).
Complete phenotypic details were available for 163 of 164 cases of Crohn disease (99.4%) and 159 of 160 cases of ulcerative colitis (99.4%). Most patients with Crohn disease were diagnosed when aged 17–40 years and had disease affecting both the ileum and colon (68 of 164 patients, 41%). Disease was usually inflammatory but non‐stricturing and non‐penetrating (98 patients, 60%); 37 patients (23%) were classified as having peri‐anal disease. The most frequent disease extent for ulcerative colitis was left‐sided colitis (63 of 160 patients, 39%) (Box 3).
Prevalence rates
The crude IBD prevalence rate was 414 cases (95% CI, 371–456 cases) per 100 000 population; the age‐standardised rate was 348 cases (95% CI, 312–385 cases) per 100 000 population. The age‐standardised prevalence of Crohn disease was slightly higher than that of ulcerative colitis (Box 4).
Age‐specific prevalence rates
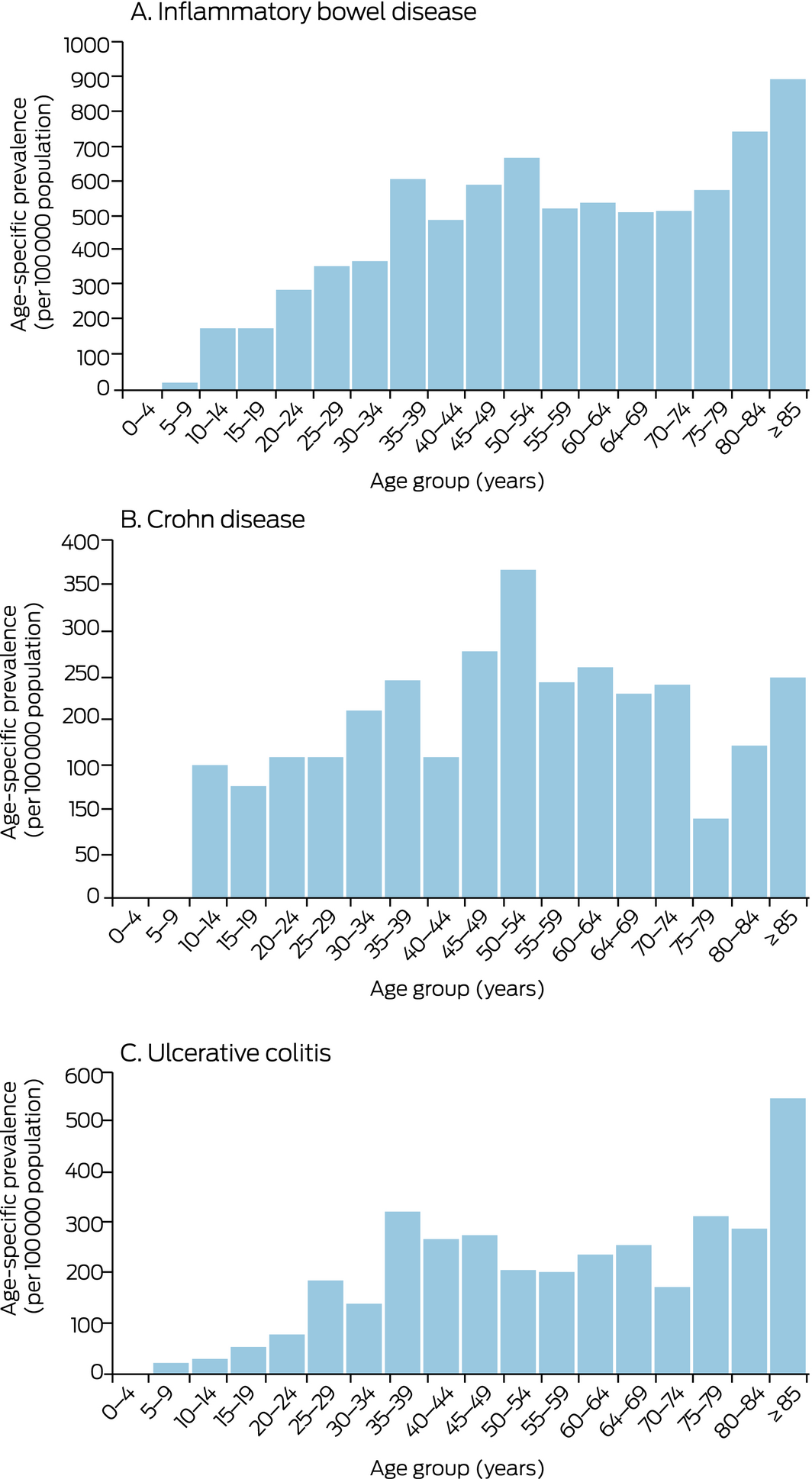
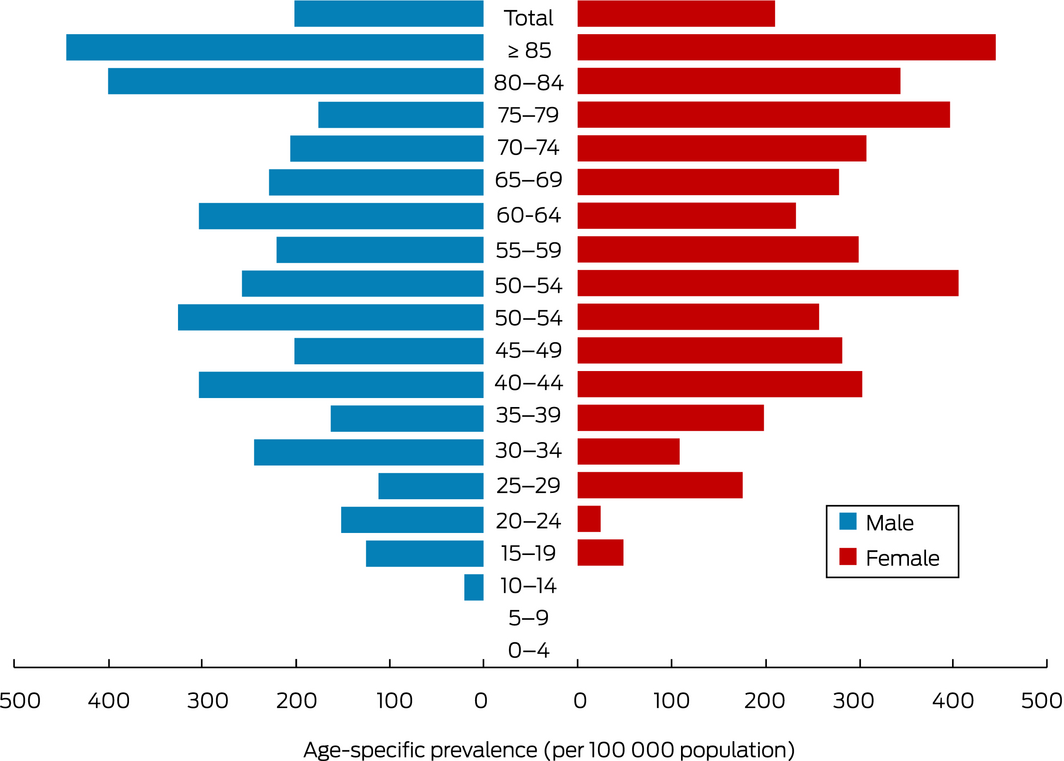
IBD prevalence increased with age (Box 5). The prevalence of Crohn disease peaked in the 50–54‐year age group, that of ulcerative colitis in the 35–39‐year and the 85 years or more age groups (Box 6). The age distribution was similar for both sexes (Box 7).
Age at diagnosis
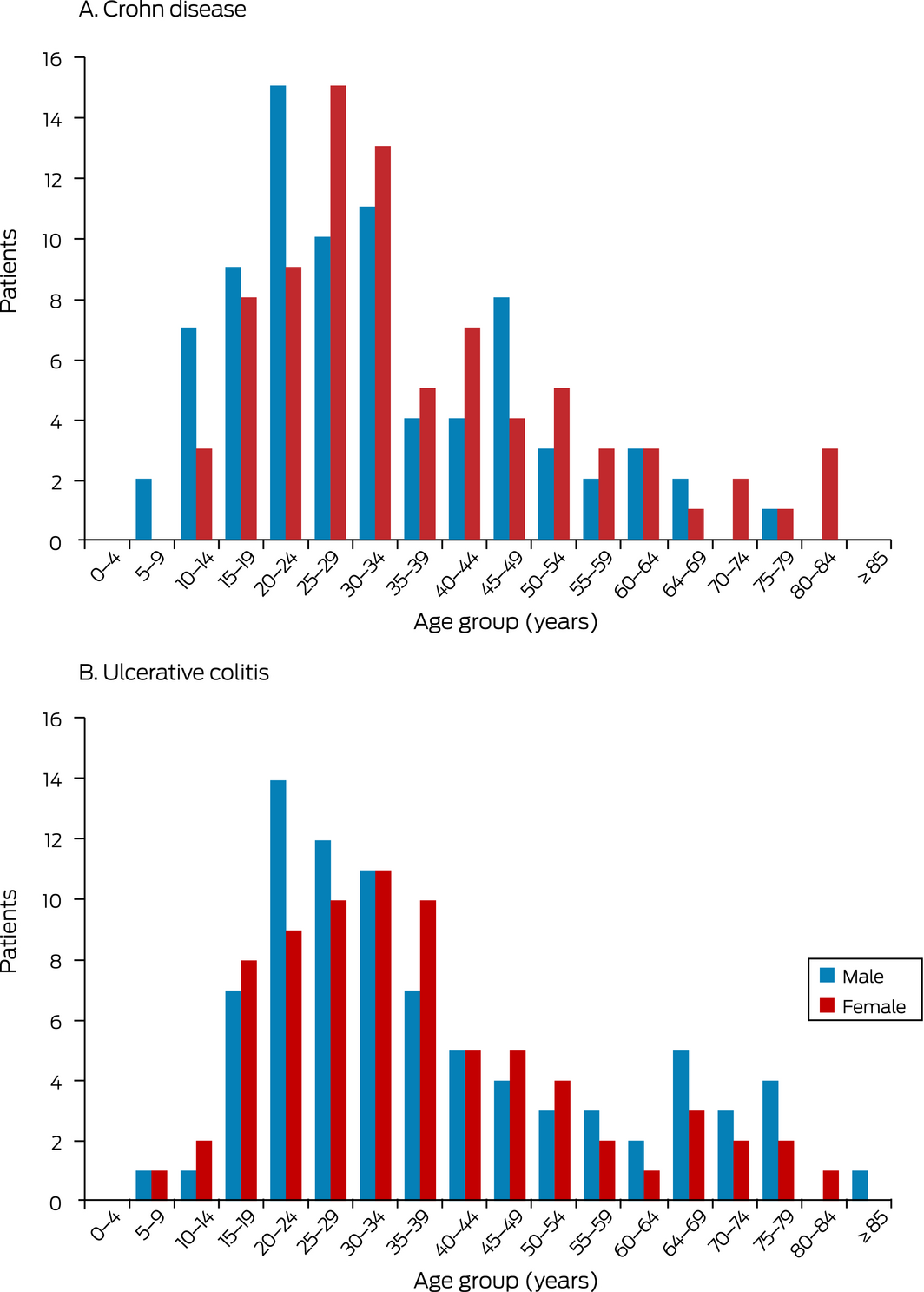
Age at diagnosis was available for 362 of 364 patients (99.5%). Median age at diagnosis was 32 years (IQR, 23–48 years). For Crohn disease, the median age of diagnosis was 27 years (IQR, 20–41.5 years) for men, 31.5 years (IQR, 25–47 years) for women. For ulcerative colitis, the median age at diagnosis was 31 years (IQR, 24–53 years) for men, 32 years (IQR, 23–46 years) for women (Box 8).
Data sources
Of the 364 cases, 175 (48%) were identified in a single data source, including 139 patients of a private gastroenterologist (Supporting Information, table 2).
Discussion
We have reported the first population‐based IBD prevalence study in New South Wales, and the first IBD prevalence study in Australia restricted to a metropolitan area. Our population‐based methodology allows direct comparison with other national and international studies (Supporting Information, table 3). We found the highest age‐standardised rates of IBD (348 cases per 100 000 population), Crohn disease (166 per 100 000 population) and ulcerative colitis (148 per 100 000 population) reported by any study in Australia or New Zealand.5,7,17 The prevalence rate of Crohn disease was higher than that of ulcerative colitis, as also found by earlier Australian, New Zealand and Canadian studies,5,7,17,18,19 but not by older studies from Scandinavia and North America.20,21,22 These differences are consistent with observations over the past fifty years that the incidence of ulcerative colitis had increased but then plateaued, while that of Crohn disease has continued to increase.23
Our prevalence rates are slightly higher than reported by earlier Australian studies for mixed urban and rural populations.5,7 The difference is probably attributable to a time‐cohort effect (cumulative increase in number of IBD cases over time), but our higher rate may be related to the urban nature of our sample. A systematic review and meta‐analysis found that the risks of Crohn disease (incidence rate ratio [IRR], 1.42; 95% CI, 1.26–1.60) and ulcerative colitis (IRR, 1.17; 95% CI, 1.03–1.32) were higher for urban than rural residents.22 Factors that may contribute to greater risk include higher rates of smoking (for Crohn disease), better hygiene and sanitation, antibiotic use, and air pollution in urban areas, as well as migration of young people from rural to metropolitan regions for education and employment. Further exploration of risk factors associated with urban living that may contribute to the pathogenesis of IBD is required.24
Our major finding was that the age‐specific prevalence of IBD increased with age. The prevalence rate among people aged 65 years or more was 612 (95% CI, 564–660 cases) per 100 000 population, and 380 (95% CI, 342–418 cases) per 100 000 people under 65 years of age; 79 patients with IBD (22%) were 65 years or more old, compared with 12 916 of 88 015 people (14.7%) in the City of Canada Bay population. We also found that the prevalence of IBD among people aged 85 years or more was 891 per 100 000 people. Both rates are higher than the 483 cases per 100 000 people age 65 years or more reported by an earlier Australian study, which found that IBD prevalence increased from the age of 15–24 years, and was highest among those aged 25–54 years and people aged 65 years or more.5 Our differing finding is probably attributable to a cumulative increase in the number of IBD cases over time.
A Canadian study found that the prevalence of ulcerative colitis was highest among people aged 40–49 years, but was similar for older age groups.19 Findings from other studies have been heterogeneous; some North American studies reported, like us, a steady increase in IBD prevalence with age, particularly of ulcerative colitis.18,22 As ulcerative colitis is more common among non‐smokers, these patients may have lower mortality, as they are healthier than the age‐matched general population, as previously reported.25
The rising prevalence of IBD with age is important for management strategies, including the use of immunosuppressive medications that exacerbate the risks of infections and malignancies in older people.26 Accurate prevalence rates allow health care administrators to efficiently plan for investigating IBD and managing patients. Our findings highlight the importance of safer therapies, appropriate cancer screening, and taking comorbid conditions into account when managing older people with IBD.27 Systemic immunosuppressive therapies should be de‐escalated when possible, and newer biological agents less likely to lead to sepsis, such as ustekinumab and vedolizumab, should be considered.26
The demographic features of the City of Canada Bay are similar to those of Greater Sydney, NSW, and Australia (Supporting Information, table 4), except for higher proportions than the Australian population of people with Chinese (17% v 5.2%) or Italian ancestry (15% v 4.3%). Extrapolating the IBD prevalence rate in Canada Bay would suggest that 16 797 people in Greater Sydney, 26 046 in NSW, and 81 485 in Australia live with IBD. By way of comparison, it was estimated in 2013 that the number of people in Australia living with IBD in 2016 would lie in the range 72 805–89 502.6
Strengths and limitations
We fully characterised all included patients to confirm diagnoses according to the Copenhagen and revised Porto criteria. Duplication of cases was avoided by uniquely identifying each case. Phenotypic details were available for all but two patients, perhaps explaining the larger proportion of IBDU patients than in other studies. In contrast, detailed information on disease location in another Australian study was available for only 350 of 579 patients with prevalent Crohn disease (60%).5
Limitations include the fact that we undertook a retrospective review of medical records, and we may have missed patients who sought gastroenterology care outside the City of Canada Bay. Mild cases of IBD may be managed by family physicians, but they do not usually manage IBD without involving a specialist gastroenterologist.28 We used different search methods to reduce selection bias, including searches of paper medical records and for keywords in electronic medical records. Further, we selected an area with a small population compared with some other studies. However, the smaller population facilitated full case ascertainment in a metropolitan area, an approach not previously undertaken in Australia. The ethnic background, socio‐economic status, and urban nature of our population may affect the generalisability of our findings to Australia as a whole. Finally, undiagnosed IBD is possible, as the median time from symptom onset to diagnosis is 4 months for ulcerative colitis and 9 months for Crohn disease.29
Conclusion
In the first IBD prevalence study in New South Wales, the most populous state in Australia, we found that its prevalence was high in the City of Canada Bay, particularly among people aged 65 years or more. The high age‐specific IBD prevalence in the middle‐aged and older people has important implications for treatment decisions.
Box 1 – The City of Canada Bay local government area
Source: City of Canada Bay Council.10 Reproduced with kind permission of the copyright holder, .id (https://home.id.com.au).
Box 2 – Demographic characteristics of residents of the City of Canada Bay with inflammatory bowel disease
|
|
|
Inflammatory bowel disease type |
|||||||||||||
|
|
All |
Crohn disease |
Ulcerative colitis |
Unspecified |
|||||||||||
|
|
|||||||||||||||
|
|
364 |
164 |
160 |
40 |
|||||||||||
|
Sex (male) |
179 (49%) |
82 (50%) |
83 (52%) |
14 (35%) |
|||||||||||
|
Age (years), median (IQR) |
47.0 (34.0–62.0) |
45.5 (31.0–56.3) |
46.5 (36.0–63.0) |
56.5 (43.3–76.0) |
|||||||||||
|
Disease duration (years), median (IQR) |
9.0 (4.0–17.0) |
8.0 (4.0–17.0) |
10.0 (4.0–18.0) |
11.0 (4.0–13.5) |
|||||||||||
|
|
|||||||||||||||
|
IQR = interquartile range. |
|||||||||||||||
Box 3 – Inflammatory bowel disease phenotypes of patients in the City of Canada Bay, according to the Montreal classification11
|
Phenotype characteristics |
|
||||||||||||||
|
|
|||||||||||||||
|
Crohn disease |
164 |
||||||||||||||
|
Age at diagnosis (years) |
|
||||||||||||||
|
< 16 |
17 (10%) |
||||||||||||||
|
17–40 |
95 (58%) |
||||||||||||||
|
> 40 |
51 (31%) |
||||||||||||||
|
Missing data |
1 |
||||||||||||||
|
Disease extent |
|
||||||||||||||
|
L1 (ileal) |
43 (26%) |
||||||||||||||
|
L2 (colonic) |
53 (32%) |
||||||||||||||
|
L3 (ileo‐colonic) |
68 (41%) |
||||||||||||||
|
L4 (isolated upper gastrointestinal involvement) |
0 |
||||||||||||||
|
Disease behaviour |
|
||||||||||||||
|
B1 (non‐stricturing and non‐penetrating) |
98 (60%) |
||||||||||||||
|
B2 (stricturing) |
34 (21%) |
||||||||||||||
|
B3 (penetrating) |
31 (19%) |
||||||||||||||
|
P (perianal involvement) |
37 (23%) |
||||||||||||||
|
Missing data |
1 |
||||||||||||||
|
Ulcerative colitis |
|
||||||||||||||
|
Disease extent |
160 |
||||||||||||||
|
E1 (proctitis) |
56 (35%) |
||||||||||||||
|
E2 (left‐sided colitis) |
63 (39%) |
||||||||||||||
|
E3 (pancolitis) |
40 (25%) |
||||||||||||||
|
Missing data |
1 |
||||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Box 4 – Prevalence of inflammatory bowel disease and its subtypes in the City of Canada Bay
|
Subtype |
Number of cases |
Crude point prevalence rate, |
Age‐standardised prevalence rate, per 100 000 (95% CI) |
||||||||||||
|
|
|||||||||||||||
|
All types |
364 |
414 (371–456) |
348 (312–385) |
||||||||||||
|
Crohn disease |
164 (45%) |
186 (158–215) |
166 (141–192) |
||||||||||||
|
Ulcerative colitis |
160 (44%) |
182 (154–210) |
148 (124–171) |
||||||||||||
|
Unspecified |
40 (11%) |
45 (31–60) |
34 (23–46) |
||||||||||||
|
|
|||||||||||||||
|
CI = confidence interval. |
|||||||||||||||
Box 5 – Age‐specific prevalence of inflammatory bowel disease in the City of Canada Bay
|
Age group (years) |
Number of cases |
Prevalence rate, |
|||||||||||||
|
|
|||||||||||||||
|
0–64 |
285 |
380 (342–418) |
|||||||||||||
|
0–4 |
0 |
0 |
|||||||||||||
|
5–9 |
1 |
21 (12–30) |
|||||||||||||
|
10–14 |
7 |
174 (146–202) |
|||||||||||||
|
15–19 |
7 |
175 (149–204) |
|||||||||||||
|
20–24 |
18 |
287 (253–320) |
|||||||||||||
|
25–29 |
29 |
354 (318–391) |
|||||||||||||
|
30–34 |
31 |
365 (327–402) |
|||||||||||||
|
35–39 |
42 |
606 (558–654) |
|||||||||||||
|
40–44 |
31 |
484 (441–527) |
|||||||||||||
|
45–49 |
34 |
586 (539–633) |
|||||||||||||
|
50–54 |
36 |
663 (612–713) |
|||||||||||||
|
55–59 |
26 |
522 (477–566) |
|||||||||||||
|
60–64 |
23 |
538 (492–583) |
|||||||||||||
|
≥ 65 |
79 |
612 (564–660) |
|||||||||||||
|
65–69 |
20 |
507 (463–551) |
|||||||||||||
|
70–74 |
15 |
512 (468–556) |
|||||||||||||
|
75–79 |
13 |
572 (526–619) |
|||||||||||||
|
80–84 |
13 |
743 (689–796) |
|||||||||||||
|
≥ 85 |
18 |
891 (833–949) |
|||||||||||||
|
|
|||||||||||||||
|
CI = confidence interval. |
|||||||||||||||
Received 11 May 2020, accepted 11 August 2020
- Aviv Pudipeddi1
- Jeffrey Liu1
- Viraj Kariyawasam1
- Thomas J Borody2
- James L Cowlishaw1
- Charles McDonald1
- Peter Katelaris3
- Grace Chapman1
- Crispin Corte4
- Daniel A Lemberg5
- Cheng H Lee6
- Anil Keshava1
- John Napoli7
- Robert Clancy2
- Webber Chan1
- Sudarshan Paramsothy1
- Rupert Leong1
- 1 Concord Repatriation General Hospital, Sydney, NSW
- 2 Centre for Digestive Diseases, Sydney, NSW
- 3 University of Sydney, Sydney, NSW
- 4 AW Morrow Gastroenterology and Liver Centre, Royal Prince Albert Hospital, Sydney, NSW
- 5 Sydney Children's Hospital, Sydney, NSW
- 6 Children's Hospital at Westmead, Sydney, NSW
- 7 Ryde Hospital, Sydney, NSW
Viraj Kariyawasam undertakes consultancy work for Janssen‐Cilag and has received grants from Takeda, Ferring, Abbvie, and Shire. Thomas Borody has a pecuniary interest in the Centre for Digestive Diseases and sits on advisory boards for Redhill, Crestovo, and Finch Therapeutics. Crispin Corte has received unrestricted research grants from Shire and Ferring, and has received speakers’ honoraria from Abbvie, Ferring, Janssen, Takeda, and Shire. Rupert Leong has served on advisory boards for AbbVie, Aspen, Celgene, Ferring, Janssen, and Takeda, and has received unrestricted research support from the National Health and Medical Research Council, Shire, and Janssen, and speakers’ honoraria from Emerge Health.
- 1. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2018; 390: 2769–2778.
- 2. Coward S, Clement F, Benchimol EI, et al. Past and future burden of inflammatory bowel disease based on modeling of population-based data. Gastroenterology 2019; 156: 1345–1353.
- 3. Ng SC, Tang W, Ching JY, et al. Asia-Pacific Crohn's and Colitis Epidemiologic Study (ACCESS) Study Group. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-Pacific Crohn’s and colitis epidemiological study. Gastroenterology 2013; 145: 158–165.
- 4. Ray K. IBD: the changing epidemiology of IBD. Nat Rev Gastroenterol Hepatol 2017; 14: 690.
- 5. Studd C, Cameron G, Beswick L, et al. Never underestimate inflammatory bowel disease: high prevalence rates and confirmation of high incidence rates in Australia. J Gastroenterol Hepatol 2016; 31: 81–86.
- 6. PricewaterhouseCoopers Australia; Crohn’s and Colitis Australia. Improving inflammatory bowel disease care across Australia. Mar 2013. https://www.crohnsandcolitis.com.au/site/wp-content/uploads/PwC-report-2013.pdf (viewed June 2019).
- 7. Bhatia R, Yeoh SW, Vaz K, et al. Inflammatory bowel disease incidence, prevalence and 12-month initial disease course in Tasmania, Australia. Intern Med J 2019; 49: 622–630.
- 8. Ng SC, Kaplan GG, Tang W, et al. Population density and risk of inflammatory bowel disease: a prospective population-based study in 13 countries or regions in Asia-Pacific. Am J Gastroenterol 2019; 114: 107–115.
- 9. Jones GR, Lyons M, Plevris N, et al. IBD prevalence in Lothian, Scotland, derived by capture-recapture methodology. Gut 2019; 68: 1953–1960.
- 10. City of Canada Bay Council. Welcome to the City of Canada Bay: community profile. Updated Oct 2016. http://profile.id.com.au/canada-bay/about (viewed Nov 2016).
- 11. Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol 2005; 19 (Suppl A): 5A–36A.
- 12. Munkholm P. Crohn’s disease: occurrence, course and prognosis. An epidemiologic cohort-study. Dan Med Bull 1997; 44: 287–302.
- 13. Langholz E. Ulcerative colitis. An epidemiological study based on a regional inception cohort, with special reference to disease course and prognosis. Dan Med Bull 1999; 46: 400–415.
- 14. Levine A, Koletzko S, Turner D, et al. European Society of Pediatric Gastroenterology, Hepatology, and Nutrition. ESPGHAN revised Porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr 2014; 58: 795–806.
- 15. Ahmad OB, Boschi-Pinot C, Lopez AD, et al. Age standardization of rates: a new WHO standard (GPE Discussion paper series: No. 31). Geneva: World Health Organization, 2001. http://who.int/healthinfo/paper31.pdf (viewed Sept 2019).
- 16. Keyfitz N. Sampling variance of standardized mortality rates. Hum Biol 1966; 38: 309–317.
- 17. Gearry RB, Richardson A, Frampton C, et al. High incidence of Crohn’s disease in Canterbury, New Zealand: results of an epidemiologic study. Inflamm Bowel Dis 2006; 12: 936–943.
- 18. Bernstein CN, Wajda A, Svenson LW, et al. The epidemiology of inflammatory bowel disease in Canada: a population-based study. Am J Gastroenterol 2006; 101: 1559–1568.
- 19. Bitton A, Vutcovici M, Patenaude V, et al. Epidemiology of inflammatory bowel disease in Quebec: recent trends. Inflamm Bowel Dis 2014; 20: 1770–1776.
- 20. Jacobsen BA, Fallingborg J, Rasmussen HH, et al. Increase in incidence and prevalence of inflammatory bowel disease in northern Denmark: a population-based study, 1978–2002. Eur J Gastroenterol Hepatol 2006; 18: 601–606.
- 21. Loftus CG, Loftus EV, Harmsen WS, et al. Update on the incidence and prevalence of Crohn’s disease and ulcerative colitis in Olmsted County, Minnesota, 1940–2000. Inflamm Bowel Dis 2007; 13: 254–261.
- 22. Kappelman MD, Rifas-Shiman SL, Kleinman K, et al. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin Gastroenterol Hepatol 2007; 5: 1424–1429.
- 23. Ng SC, Bernstein CN, Vatn MH, et al; Epidemiology and Natural History Task Force of the International Organization of Inflammatory Bowel Disease (IOIBD). Geographical variability and environmental risk factors in inflammatory bowel disease. Gut 2013; 62: 630–649.
- 24. Soon IS, Molodecky NA, Rabi DM, et al. The relationship between urban environment and the inflammatory bowel diseases: a systematic review and meta-analysis. BMC Gastroenterol 2012; 12: 51.
- 25. Selinger CP, Andrews J, Dent OF, et al. Cause-specific mortality and 30-year relative survival of Crohn’s disease and ulcerative colitis. Inflamm Bowel Dis 2013; 19: 1880–1888.
- 26. Pudipeddi A, Kariyawasam V, Haifer C, et al. Safety of drugs used for the treatment of Crohn’s disease. Expert Opin Drug Saf 2019; 18: 357–367.
- 27. Kariyawasam VC, Kim S, Mourad FH, et al. Comorbidities rather than age are associated with the use of immunomodulators in elderly-onset inflammatory bowel disease. Inflamm Bowel Dis 2018; 25: 1390–1398.
- 28. Tan M, Holloway RH, Lange K, et al. General practitioners’ knowledge of and attitudes to inflammatory bowel disease. Intern Med J 2012; 42: 801–807.
- 29. Vavricka SR, Spigaglia SM, Rogler G, et al. Systematic evaluation of risk factors for diagnostic delay in inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: 496–505.
Abstract
Objectives: To determine the age‐standardised prevalence of inflammatory bowel disease (IBD) in a metropolitan area of Sydney, with a focus on its prevalence among older people.
Design, setting: Population‐based epidemiological study of people with IBD in the City of Canada Bay, a local government area in the inner west of Sydney, during 1 March 2016 – 10 November 2016.
Participants: Patients diagnosed with confirmed IBD according to the Copenhagen or revised Porto criteria.
Main outcome measures: Crude prevalence of IBD, including Crohn disease and ulcerative colitis; age‐standardised prevalence of IBD, based on the World Health Organization standard population; prevalence rates among people aged 65 years or more.
Results: The median age of 364 people with IBD was 47 years (IQR, 34–62 years); 185 were women (50.8%). The crude IBD prevalence rate was 414 cases (95% CI, 371–456 cases) per 100 000 population; the age‐standardised rate was 348 cases (95% CI, 312–385 cases) per 100 000 population. The age‐standardised rate for Crohn disease was 166 cases (95% CI, 141–192 cases) per 100 000 population; for ulcerative colitis, 148 cases (95% CI, 124–171 cases) per 100 000 population. The IBD prevalence rate in people aged 65 years or more was 612 cases (95% CI, 564–660 cases) per 100 000, and for those aged 85 years or more, 891 cases (95% CI, 833–949 cases) per 100 000; for people under 65, the rate was 380 cases (95% CI, 342–418 cases) per 100 000.
Conclusions: We found that the prevalence of confirmed IBD in a metropolitan sample was highest among older people. Challenges for managing older patients with IBD include higher rates of comorbid conditions, polypharmacy, and cognitive decline, and the immunosuppressive nature of standard therapies for IBD.