




Increasing numbers of women are graduating in medicine in Australia1 and overseas.2,3 This has led to a “feminisation of medicine”,4 and concerns have been expressed that women work fewer hours than men, primarily because of family commitments.5 Such criticism focuses on the competing demands of being mothers and doctors, and the career breaks taken by women to care for children.4
Balancing the two roles can be challenging. Doctors must prioritise patient care, often to the detriment of their own needs and those of their families.6,7 Motherhood can be as personally rewarding as medicine, and similarly requires placing another person's needs before one's own.8 In this systematic review, we identify what is known about women balancing motherhood and medicine by examining the published research into their experiences and perspectives.
Methods
Search strategy
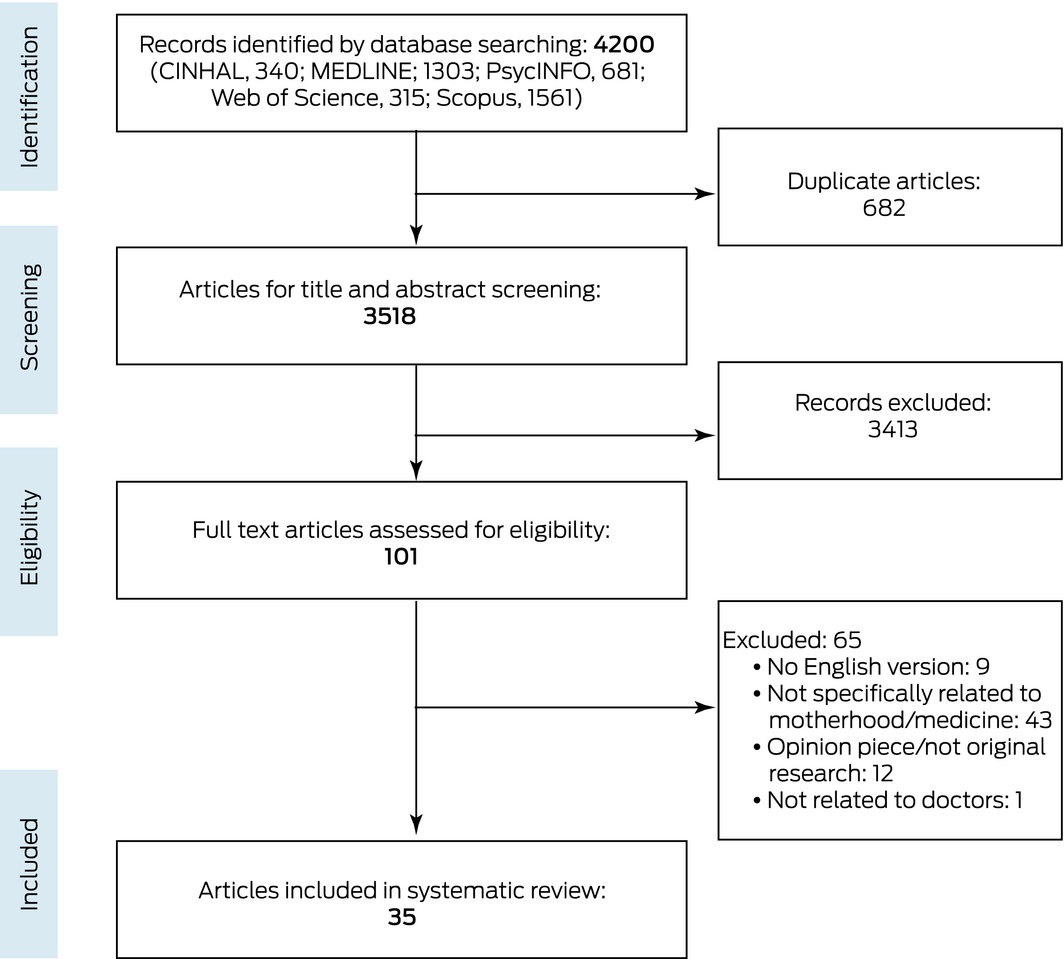
Our systematic review was prospectively registered with PROSPERO on 30 April 2019 (CRD42019116228). We searched the CINAHL (Cumulative Index to Nursing and Allied Health Literature), MEDLINE, PsycINFO, Web of Science, and Scopus databases in November 2019 for relevant published studies with the same search string: female/women AND doctor*/physician*/clinician* AND family OR child* OR mother* OR parent AND “family work relationships” OR “work life balance” OR “work home culture” (Supporting Information, table 1).
Study selection and data extraction
The titles and abstracts of articles identified by our search were screened by two authors (RH, MN), and the full text of relevant articles were then assessed according to our inclusion criteria:
- published during 2008–2019;
- full text was available in English;
- the publication described original research;
- the publication had been peer‐reviewed;
- the study population included medical doctors;
- the study examined women's experiences, or women/female sex was a variable in the study;
- the study examined a component of parenthood.
Articles were excluded if doctors were not explicitly objects of the study, sex was not a variable in the study, or motherhood or parental experiences were not reviewed. Disagreements about inclusion were resolved by consensus between the two authors.
Screening identified 101 potentially relevant articles. After excluding nine because no English language versions were available, 43 not specifically related to motherhood or medicine, one undergraduate study not about doctors, and twelve non‐research articles, 35 original research studies were included in our systematic review (Box 1).
Thematic analysis
We undertook an integrative review synthesis of the included research studies. Information was categorised according to emergent themes and synthesised. A quantitative meta‐analysis was not attempted because of marked differences between studies in the outcomes and variables assessed.
Results
Nineteen of the 35 research studies (32 quantitative, three qualitative studies) were from the United States, and three each from Japan and Germany. The quantitative studies were either cross‐sectional surveys or longitudinal in design (32 to 10 866 participants each) from specific specialities to large multi‐centre studies. The qualitative studies included focus groups and semi‐structured interviews (eight to twenty participants each) (Box 2; Supporting Information, tables 2–4).
All 35 included studies were appraised by one author (RH) with the Joanna Briggs Institute Critical Appraisal tools9 and deemed to be of moderate quality. No study included a matched comparison group, and only one10 included longitudinal follow‐up of a cohort of women.
Three core themes were identified by thematic analysis:
- Motherhood: the impact of being a doctor on raising children;
- Medicine: the impact of being a mother on a medical career; and
- Combining motherhood and medicine: strategies and policies.
1. Motherhood: the impact of being a doctor on raising children
The first theme, derived from one qualitative study (20 participants)10 and ten quantitative cross‐sectional surveys (183 to 6880 participants),8,11,12,13,14,15,16,17,18,19 was the influence of a medical career on decisions and priorities related to motherhood, including decisions about whether to have children, and when and how many, as well as the ongoing effect of a medical career on a woman's family (Supporting Information, table 2).
Five studies reported that women who were doctors described decisions about having children or pursuing career progression as difficult.10,12,13,16,18 Most participating women reported prioritising their careers, including completion of specialty training, by choosing to delay having children.10,13,16,18 In one study,12 513 of 801 respondents (64%) deferred having children for career reasons. Other studies similarly found that women delayed having families to attain specific career goals.11,12,14,19 Female surgeons in the US were twice as likely as male surgeons to delay having children until after postgraduate residency training; women who had children early in their career felt less financially secure and more anxious than women who commenced families later in their career.16 In another study, women who had children during training reported greater family strain than women who did not have children.17
Decisions about career progression influence family size; for instance, an Egyptian study found that 247 of 300 women (82%) had smaller families because they had decided to prioritise their advancement as physicians.19 Two other studies found that a smaller family was a possible consequence of deferring pregnancy for career reasons,11,12 highlighted by the remark: “I [deferred] having a second child. Never got to it. Big regret in my life.”12 Shift work and certain specialisation choices (such as dermatology)14 were also found to influence family size.
Several studies found that a medical career could have a negative impact on family life and relationships.8,14,15,16,17,19 For example, two US studies identified that the working hours of women surgeons caused family strain;16,17 another found that 2071 of 5582 female doctors (37%) believed that their career negatively affected relationships with their children.15 Similarly, 36 of 91 female dermatologists with children (40%) felt that they had missed their children's milestones because of their careers.14
2. Medicine: the impact of being a mother on a medical career
The second theme, derived from 17 quantitative studies (32 to 10 866 participants)8,13,19,20,21,22,23,24,25,26,27,28,29,30,32,33,34 and one qualitative study (eight participants),31 was the impact of being a mother on working as a doctor (Supporting Information, table 3).
There were two subthemes. The first was the effect of the responsibilities and preferences associated with pregnancy and parenthood on career motivation. Four studies found that motherhood did not reduce the motivation and ability of female doctors to return to work.13,20,32,33 A Dutch study found that female doctors who wanted or already had children remained motivated to work;33 a Swiss study found that 78 of 109 female doctors (72%) continued working more than half‐time after having children.32 Similar findings were reported by British13 and Latin American studies20 in which respectively 47% and 54% of female doctors sought work in family‐friendly environments (generalist or primary care settings).
The number of hours worked after maternity leave was influenced by childcare availability, personal and family preferences, and working arrangements.8,19,27,28,34 A Japanese survey (224 respondents) found that 38% of female surgeons changed their work plans to accommodate childcare; further, acute childhood illnesses, educational activities, and parenting responsibilities affected decisions about work, and 11% had resigned their jobs.27 Time required for parenting also affected working hours.19,21,23,25,29 Two US studies reported that female surgeons undertook a greater share of childcare planning and domestic activities than male surgeons.21,25 A multinational study similarly found that women bore greater responsibility for parenting and domestic roles than men in the same surgical specialty.29
The second subtheme concerned perceptions of pregnancy and motherhood, discussed in four studies from the viewpoint of the colleagues of female doctors and program directors.23,24,26,30 In three studies, conducted in the Lebanon,23 South Africa,24 and the US,26 doctors reported that their workloads were greater when working alongside pregnant doctors, and they rated pregnant colleagues as less productive.23 The US study also found that ten of 22 program directors (45%) reported that their hiring decisions were influenced by disclosures by potential employees regarding pregnancy or pregnancy plans;23 it was unclear whether this reflected policies on pregnancy in training positions, or personal beliefs about pregnant doctors. According to a longitudinal cohort study, negative perceptions of pregnant colleagues have improved in the US; the authors found that support from program directors and faculty staff for hiring and retaining female doctors had increased during 2008–2015.26
Female doctors reported perceptions of gender bias; for example, a surgical training registrar commented that “women are not taken seriously, as they may soon get pregnant.”24 A qualitative study in the US found that female doctors were often presumed to be disinterested, unavailable, or unwilling to complete tasks, work extra hours, or be promoted if they had children; one participant stated that colleagues thought that “you don't want to deal with that: you have small kids.”22
3. Combining motherhood and medicine: strategies and policies
The final theme, derived from two qualitative studies31,40 (eight participants each), and ten quantitative studies (45 to 546 participants),14,30,35,36,37,38,39,41,42,43 concerned the strategies and policies for assisting women balance motherhood and a medical career (Supporting Information, table 4).
Maternity leave and policies on leave and career progression directly influenced the ability of women to balance motherhood and medical careers.14,30,35,37 A US study found that 89 of 96 female dermatologists (93%) took less than three months’ maternity leave after giving birth; 24 (25%) had returned to work within a month.14 In another US survey, 251 of 320 female surgeons (78%) took less than six weeks’ maternity leave, and 250 of 347 (72%) thought the duration of leave inadequate.37 That the American Board of Surgery allows a total of only six weeks’ leave, including annual and maternity leave, was cited in one study as one reason for this situation; a participant commented that surgery “is hard, being a mum is hard … I gave up all of my vacation for maternity leave … [that] hurt my morale and spirit the most.”35 A German article discussed how hospital policies discouraged women from working in surgery when pregnant, causing them to disclose pregnancies late or to retire from theatre surgery.30
Several studies described strategies for assisting women balance motherhood and medicine.31,36,39,40,42,43 Strategies included workplaces with policies for expanded childcare and breastfeeding facilities or otherwise promoted flexibility in the workplace.39,42 In a survey of paediatricians (546 respondents), 88% reported their residency programs included maternity leave policies; 63% reported flexible rostering, 24% on‐site childcare, and 51% lactation rooms.43 This study also found that child‐friendly workplaces and those with flexible policies were deemed to be more attractive as training locations.43
The few studies that have evaluated pregnancy and maternity leave policies have been conducted in the US.36,38,41 Thirty‐three of 52 plastic surgery residency programs did not have formal maternity leave policies (63%);38 there was no identified national maternity or paternity policy for orthopaedic surgeons, and hospital and training programs had policies that were often not implemented.41 Further, program directors from a range of specialties commented that 137 of 298 programs (46%) did not adequately support women during pregnancy and parenting.36 Similarly, surgical residents reported that maternity support and policies were inadequate.35
Discussion
Our systematic review provides insights into possible barriers and facilitators for women striving to balance their aspirations for both a medical career and family. The key themes identified indicate the diversity of factors that affect pursuing the dual careers of mother and doctor. It was often reported that women prioritise career advancement by delaying starting a family.10,12,13 Women who have completed higher education in areas other than medicine are similarly likely to delay pregnancy and motherhood until their thirties; in an American survey, more than 50% of women with tertiary educations had their first children after the age of 30, while 64% of women with first pregnancies before age 25 had not completed high school.44 Delaying having children may affect a woman's ability to conceive, increases the risks of complications during pregnancies, and increases the risks of mother and child requiring medical interventions.45 These implications may not be considered by women when giving priority to career opportunities.
Some studies reported that female doctors believed that career progression would be slowed by motherhood,28,29 similar to findings in other professions. In business careers, for example, leaves of absence have been associated with fewer promotions and poorer annual review outcomes,46 especially for women who take leave of absence to have children;47 in managerial positions, each year of delayed motherhood was found to increase earnings by 9%.48 The perception that women should be at home providing childcare is a barrier to career progression in many professions.49 Strategies for overcoming this problem include education and targeted leadership development programs,50 but research specific to medical practice is needed. Few evaluations of policies for supporting pregnant doctors, providing maternity leave, and assisting their return to work after giving birth have been published. There is, however, some evidence that trainees prefer programs that provide maternity leave and offer flexible return‐to‐work strategies.39,42
Limitations
The methodological quality of the included articles was moderate. Most described single cohort studies, only one of which was a longitudinal study. Most investigations focused on hospital‐based specialties and were restricted to single hospitals or specialty training programs, with only limited consideration of community‐based specialties such as general practice. Specific cultural and religious factors that can influence choices related to motherhood and career were not investigated. We found no relevant studies conducted in Australia or New Zealand. A final limitation was that we excluded studies for which English language versions were not available.
Conclusion
Notable barriers to women pursuing both a medical career and motherhood have been identified. Prospective studies and rigorous evaluations of policies and support mechanisms in different medical specialties should be undertaken. As more than one‐half of medical trainees are women, the dual roles of mother and medical practitioner need to be considered in greater depth, with a view to establishing sustainable strategies that enable women to excel in both roles.
Box 1 – Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow diagram of article selection for our review
Box 2 – Summary of articles included in our systematic review, by identified themes
|
Study |
Year |
Country |
Design |
Focus |
Participants |
Theme* |
|||||||||
|
|
|||||||||||||||
|
Hill11 |
2018 |
US |
Quantitative survey |
Timing and size of family |
677 doctors |
1 |
|||||||||
|
Bering12 |
2018 |
US |
Quantitative survey |
Deferred personal life decisions by female doctors |
801 doctors |
1 |
|||||||||
|
Kawase8 |
2018 |
JP |
Quantitative survey |
Personal life priorities |
6211 surgeons |
1,2 |
|||||||||
|
Lambert13 |
2017 |
UK |
Quantitative survey |
Impact of having children on specialty choice |
2057 doctors |
1,2 |
|||||||||
|
Reimann10 |
2017 |
DE |
Qualitative |
Choice to be mother or doctor |
20 female doctors |
1 |
|||||||||
|
Mattessich14 |
2017 |
US |
Quantitative survey |
Career options for female dermatologists |
183 dermatologists |
1,3 |
|||||||||
|
Shanafelt15 |
2016 |
US |
Quantitative survey |
Parental satisfaction |
6880 doctors |
1 |
|||||||||
|
Chen16 |
2013 |
US |
Quantitative survey |
Effects of marriage and childbirth |
4028 residents |
1 |
|||||||||
|
Sullivan17 |
2013 |
US |
Quantitative survey |
Effects of marriage and childbirth |
4402 residents |
1 |
|||||||||
|
Estryn‐Behar18 |
2011 |
FR |
Quantitative survey |
Career barriers to parenthood |
1924 doctors |
1 |
|||||||||
|
Farahat19 |
2009 |
EG |
Quantitative survey |
Challenges for female doctors |
300 doctors |
1,2 |
|||||||||
|
Lopez Leon20 |
2019 |
Latin America |
Quantitative survey |
Effect of specialty on choosing to have children |
1241 female doctors |
2 |
|||||||||
|
Ly21 |
2018 |
US |
Quantitative survey |
Time spent on household activities |
565 doctors |
2 |
|||||||||
|
Halley22 |
2018 |
US |
Quantitative survey |
Mothers’ experience of workplace discrimination |
947 doctors |
2 |
|||||||||
|
Attieh23 |
2018 |
LB |
Quantitative survey |
Pregnancy during residency |
89 residents, 11 department heads |
2 |
|||||||||
|
Umoetok24 |
2017 |
ZA |
Quantitative survey |
Impact of sex on training and practice of surgery |
32 female surgeons |
2 |
|||||||||
|
Baptiste25 |
2017 |
US |
Quantitative survey |
Work–life balance and role responsibility |
127 faculty members, 116 trainees |
2 |
|||||||||
|
Mundschenk26 |
2016 |
US |
Quantitative survey |
Support for pregnant women during residency |
203 female doctors |
2 |
|||||||||
|
Fujimaki27 |
2016 |
JP |
Quantitative survey |
Influence of life events |
244 neurosurgeons, 469 chief surgeons |
2 |
|||||||||
|
Lachish28 |
2016 |
UK |
Quantitative survey |
Factors that influence working less than full‐time |
10 866 doctors |
2 |
|||||||||
|
Kawase29 |
2016 |
JP, US, FI, HK |
Quantitative survey |
Career barriers for female surgeons |
225 surgeons |
2 |
|||||||||
|
Knieper30 |
2014 |
DE |
Quantitative survey |
Pregnancy and surgery |
164 female doctors |
2,3 |
|||||||||
|
Schueller‐Weidekamm31 |
2012 |
DE |
Qualitative |
Work–life balance and leadership |
8 female doctors in leadership positions |
2,3 |
|||||||||
|
Stamm32 |
2011 |
CH |
Quantitative survey |
Family structures and impact on career |
414 doctors |
2 |
|||||||||
|
Pas33 |
2011 |
NL |
Quantitative survey |
Influence of having children on career motivation |
1070 female doctors |
2 |
|||||||||
|
Buddeberg‐Fischer34 |
2010 |
CH |
Quantitative survey |
Impact of becoming a parent on career |
579 doctors |
2 |
|||||||||
|
Rangel35 |
2018 |
US |
Thematic analysis of open‐ended survey responses |
Pregnancy and surgical medicine |
219 surgical residents |
3 |
|||||||||
|
Morris36 |
2018 |
US |
Quantitative survey |
Parenting support programs |
297 program directors |
3 |
|||||||||
|
Rangel37 |
2018 |
US |
Quantitative survey |
Pregnancy during surgical training |
347 women surgeons |
3 |
|||||||||
|
Garza38 |
2017 |
US |
Quantitative survey |
Policies for plastic surgery residents |
54 plastic surgery directors |
3 |
|||||||||
|
Arima39 |
2016 |
JP |
Quantitative survey |
Work–life balance |
439 doctors |
3 |
|||||||||
|
Morris40 |
2016 |
US |
Qualitative |
Competing demands as parent and resident |
8 residents |
3 |
|||||||||
|
Weiss41 |
2016 |
US |
Quantitative survey |
Maternity/paternity/adoption leave policies in orthopaedic medicine |
45 program directors |
3 |
|||||||||
|
Pas42 |
2011 |
NL |
Quantitative survey |
Human resources strategies for doctors with children |
483 doctors |
3 |
|||||||||
|
Berkowitz43 |
2010 |
US |
Quantitative survey |
Family‐friendly aspects of the workplace |
546 doctors |
3 |
|||||||||
|
|
|||||||||||||||
|
CH = Switzerland; DE = Germany; EG = Egypt; FI = Finland; FR = France; HK = Hong Kong; JP = Japan; LB = Lebanon; NL = Netherlands; UK = United Kingdom; US = United States; ZA = South Africa. * 1. Motherhood: the impact of being a doctor on raising children; 2. Medicine: the impact of being a mother on a medical career; 3. Combining motherhood and medicine: strategies and policies. |
|||||||||||||||
Received 10 January 2020, accepted 3 March 2020
- Rebekah Hoffman1
- Judy Mullan1
- Marisa Nguyen1
- Andrew D Bonney1
- Graduate School of Medicine, University of Wollongong, Wollongong, NSW
We thank University of Wollongong librarian Brian Kenady for his guidance and the time taken to developing our search strategy.
No relevant disclosures.
- 1. Joyce CM, Scott A, Jeon SH, et al. The “Medicine in Australia: Balancing Employment and Life (MABEL)” longitudinal survey: protocol and baseline data for a prospective cohort study of Australian doctors’ workforce participation. BMC Health Ser Res 2010; 10: 50.
- 2. Jefferson L, Bloor K, Maynard A. Women in medicine: historical perspectives and recent trends. Br Med Bull 2015; 115: 5–15.
- 3. Russo G, Gonçalves L, Craveriro I, Dussault G. Feminization of the medical workforce in low‐income settings: findings from surveys in three African capital cities. Hum Resour Health 2015; 13: 64.
- 4. Brooks PM, Lapsley HM, Butt DB. Medical workforce issues in Australia: “tomorrow's doctors — too few, too far”. Med J Aust 2003; 179: 206–208. https://www.mja.com.au/journal/2003/179/4/medical-workforce-issues-australia-tomorrows-doctors-too-few-too-far.
- 5. McKinstrey B. Are there too many female medical graduates? Yes. BMJ 2008; 336: 748.
- 6. American Academy of Family Practice. Is a career in medicine right for you? [website]. Undated. https://www.aafp.org/students-residents/medical-students/considering-medical-school/is-career-in-medicine-for-you.html (viewed July 2020).
- 7. Manson A. Medicine as a vocation. J Gen Intern Med 1990; 5: 175–177.
- 8. Kawase K, Nomura K, Tominaga R, et al. Analysis of gender based differences among surgeons in Japan: results of a survey conducted by the Japan Surgical Society. Part 2: personal life. Surg Today 2018; 48: 308–319.
- 9. Aromataris E, Fernandez R, Godfrey CM, et al. Summarizing systematic reviews: methodological development, conduct and reporting of Umbrella review approach. Int J Evid Based Heal 2015; 13: 132–140.
- 10. Reimann S, Alfermann D. Female doctors in conflict: how gendering processes in German hospitals influence female physicians’ careers. Gender Issues 2018; 35: 52–70.
- 11. Hill EK, Stuckley A, Fiascone S, et al. Gender and the balance of parenting and professional life among gynaecology subspecialists. J Minim Invasive Gynecol 2019; 26: 1088–1094.
- 12. Bering J, Pflibsen L, Eno C, Radhakrishnan P. Deferred personal life decisions of women physicians. J Womens Health (Larchmt) 2018; 27: 584–589.
- 13. Lambert TW, Smith F, Goldacre MJ. Combining parenthood with a medical career: questionnaire survey of the UK medical graduated of 2002 covering some influences and experiences. BMJ Open 2017; 7: e016822.
- 14. Mattessich S, Shea K, Whitaher‐Worth D. Parenting and female dermatologists’ perceptions of work–life balance. Int J Womens Dermatol 2017; 3: 127–130.
- 15. Shanafelt TD, Hasan O, Hayes S, et al. Parental satisfaction of US physicians: associated factors and comparison with the general US working population. BMC Med Educ 2016; 16: 228.
- 16. Chen MM, Yeo HL, Roman SA, et al. Life events during surgical residency have different effects on women and men over time. Surgery 2013; 154: 162–170.
- 17. Sullivan MC, Yeo H, Roman SA, et al. Striving for work–life balance effect of marriage and children in the experience of 4402 US general surgery residents. Ann Surg 2013; 257: 571–576.
- 18. Estryn‐Behar M, Fry C, Guetarni K, et al. Work week duration, work–family balance and difficulties encountered by female and male physicians: results from the French SESMAT study. Work 2011; 40: S83–S100.
- 19. Farahat FM. Challenges facing female physicians in Egypt. Arch Environ Occup Health 2009; 64: 121–128.
- 20. Lopez Leon L, Del Valle CA, Salceda AH, et al. Medical careers and motherhood: a cross‐sectional study of Hispanic female physicians. J Grad Med Educ 2019; 11(4 Suppl): 181–185.
- 21. Ly DP, Jena AB. Sex differences in time spent on household activities and care of children among US physicians, 2003–2016. Mayo Clin Proc 2018; 93: 1484–1487.
- 22. Halley MC, Rustagi AS, Torres JS, et al. Physician mothers’ experience of workplace discrimination: a qualitative analysis. BMJ 2018; 363: k4926.
- 23. Attieh E, Maalouf S, Chalfoun C, et al. Impact of female gender and perspectives of pregnancy on admission in residency programs. Reprod Health 2018; 15: 121.
- 24. Umeotok F, Van Wyk JM, Madiba TE. Does gender impact on female doctors’ experiences in the training and practice of surgery? A single centre study. South African J Surg 2017; 55: 8–12.
- 25. Baptiste D, Fecher AM, Dolejs SC, et al. Gender differences in academic surgery, work‐life balance, and satisfaction. J Surg Res 2017; 218: 99–107.
- 26. Mundschenk MB, Krauss EM, Poppler LH, et al. Resident perceptions on pregnancy during training: 2008 to 2015. Am J Surg 2016; 212: 649–659.
- 27. Fujimaki T, Shibui S, Kato Y, et al. Working conditions and lifestyle of female surgeons affiliated to the Japan Neurosurgical Society: findings of individual and institutional surveys. Neurol Med Chir 2016; 56: 704–708.
- 28. Lachish S, Svirko E, Goldacre MJ, Lambert T. Factors associated with less than full‐time working in medical practice: results of surveys of five cohorts of UK doctors, 10 years after graduation. Hum Resour Health 2016; 14: 62.
- 29. Kawase K, Carpelan‐Holmström M, Kwong A, Sanfey H. Factors that can promote or impede the advancement of women as leaders in surgery: results from an international survey. World J Surg 2016; 40: 258–266.
- 30. Kneiper C, Ramsauer B, Hancke K, et al. “Pregnant and operating”. Evaluation of a Germany‐wide survey among female gynaecologists and surgeons. Geburtshilfe Frauenheilkd 2014; 74: 875–880.
- 31. Schueller‐Weidekamm C, Kautzy‐Willer A. Challenges of work–life balance for women physicians/mothers working in leadership positions. Gend Med 2012; 9: 244–250.
- 32. Stamm M, Biddeberg‐Fischer B. How do physicians and their partners co‐ordinate their careers and private lives? Swiss Med Wkly 2011; 141: w13179.
- 33. Pas B, Peters P, Eisinga R, et al. Explaining career motivation among female doctors in the Netherlands: the effect of children, views on motherhood and work‐home cultures. Work Employment Society 2011; 25: 487–505.
- 34. Buddeberg‐Fischer B, Stamm M, Buddeberg C, et al. The impact of gender and parenthood on physicians’ careers: professional and personal situation seven years after graduation. BMC Health Serv Res 2010; 10: 40.
- 35. Rangel EL, Castillo‐Angeles M, Changala M, et al. Perspectives of pregnancy and motherhood among general surgery residents: a qualitative analysis. Am J Surg 2018; 216: 754–759.
- 36. Morris LE, Lindbloom E, Kruse RL, et al. Perceptions of parenting residents among family medicine residency directors. Fam Med 2018; 50: 756–762.
- 37. Rangel EL, Smink DS, Castillo‐Angeles M, et al. Pregnancy and motherhood during surgical training. JAMA Surg 2018; 153: 644–652.
- 38. Garza RM, Weston JS, Furnas HJ. Pregnancy and the plastic surgery resident. Plas Reconstr Surg 2017; 139: 245–252.
- 39. Arima M, Araki Y, Iseki S, et al. Seeking a “career” and “family”: factors of satisfaction in work–life balance among child‐rearing female physicians in Japan, comparison between female physicians without children and male physicians. Health Sci J 2016; 10(4): 16.
- 40. Morris L, Cronk NJ, Washington KT. Parenting during residency: providing support for Dr mom and Dr dad. Fam Med 2016; 48: 140–144.
- 41. Weiss J, Teuscher D. What provisions do orthopaedic programs make for maternity, paternity and adoption leave? Clin Orthop Relat Res 2016; 474: 1945–1949.
- 42. Pas B, Peters P, Doorewaard H, et al. Feminisation of the medical profession: a strategic HRM dilemma? The effects of family‐friendly HR practices on female doctors’ contracted working hours. Hum Resour Manag J 2011; 21: 285–302.
- 43. Berkowitz CD, Frintner MP, Cull WL. Pediatric resident perceptions of family‐friendly benefits. Acad Pediatr 2010; 10: 360–366.
- 44. Livingston G, Cohn D. Childlessness up among all women; down among women with advanced degrees. Washington (DC): Pew Research Center, 2010. https://www.pewsocialtrends.org/2010/06/25/childlessness-up-among-all-women-down-among-women-with-advanced-degrees/#differences-by-education (viewed Oct 2019).
- 45. Waldenström U. Postponing parenthood to advanced age. Ups J Med Sci 2016; 121: 235–243.
- 46. Judiesch MK, Lyness KS. Left behind? The impact of leaves of absence on managers’ career success. Acad Manag J 1999; 42: 641–651.
- 47. Adda J, Dustmann C, Stevens K. The career costs of children. J. Polit Econ 2017; 125: 293–337.
- 48. Miller AR. The effects of motherhood timing on career path. J Popul Econ 2011; 24: 1071–1100.
- 49. Pringle JK, Harris C, Ravenswood K, et al. Women's career progression in law firms: views from the top, views from below. Gend Work Organ 2017; 24: 435–499.
- 50. Cebeza‐García L, Del Brio EB, Rueda C. Legal and cultural factors as catalysts for promoting women in the boardroom. BRQ Bus Res Q 2019; 22: 56–67.
Abstract
Objective: To synthesise what is known about women combining motherhood and a career in medicine by examining the published research into their experiences and perspectives.
Study design: We reviewed peer‐reviewed articles published or available in English reporting original research into motherhood and medicine and published during 2008–2019. Two researchers screened each abstract and independently reviewed full text articles. Study quality was assessed.
Data sources: CINAHL, MEDLINE, PsycINFO, Web of Science, and Scopus abstract databases.
Data synthesis: The database search identified 4200 articles; after screening and full text assessment, we undertook an integrative review synthesis of the 35 articles that met our inclusion criteria.
Conclusions: Three core themes were identified: Motherhood: the impact of being a doctor on raising children; Medicine: the impact of being a mother on a medical career; and Combining motherhood and medicine: strategies and policies. Several structural and attitudinal barriers to women pursuing both medical careers and motherhood were identified. It was often reported that women prioritise career advancement by delaying starting a family, and that female doctors believed that career progression would be slowed by motherhood. Few evaluations of policies for supporting pregnant doctors, providing maternity leave, and assisting their return to work after giving birth have been published. We did not find any relevant studies undertaken in Australia or New Zealand, nor any studies with a focus on community‐based medicine or intervention studies. Prospective investigations and rigorous evaluations of policies and support mechanisms in different medical specialties would be appropriate.
Protocol registration: PROSPERO CRD42019116228.