





Medical education
Lessons from practice
Volume 213 - Issue 5
The dangers of herbal teas: hypertension and weakness caused by liquorice‐induced apparent mineralocorticoid excess
Authors: Ravind Pandher, Anita Puvanendran and Terrence H Diamond
Med J Aust 2020; 213 (5): 207-208.e1. || doi: 10.5694/mja2.50728
Published online: 7 September 2020
Published online: 7 September 2020
A 51-year-old post-menopausal woman presented with a 6- week
history of headaches, nausea and vomiting, and mild lower limb oedema
Clinical record
A 51‐year‐old post menopausal woman presented to our emergency department with a 6‐week history of headaches, nausea and vomiting, and mild lower limb oedema. She was not taking any prescribed medications but had been consuming a naturopath‐prescribed herbal tea containing liquorice root, reportedly to assist with fertility. She consumed 800–1000 mL of the self‐formulated tea 6 days a week for 3 months, averaging 60 g of liquorice root per serve. Other ingredients of the tea included cinnamon bark, ginger, codonopsis, red date and morinda root.
On admission, she was found to be hypertensive (150/88 mmHg). Baseline biochemistry (Box 1) revealed a potassium level of 2.5 mmol/L (reference interval [RI], 3.5–5.2 mmol/L) and a compensated metabolic alkalosis (pH, 7.41 [RI, 7.35–7.45]; Pco2, 60 mmHg [RI, 35–45 mmHg]; bicarbonate, 37.7 mmol/L [RI, 22–32 mmol/L]) consistent with primary aldosteronism. Further investigations showed undetectable plasma aldosterone and renin levels < 27 pmol/L (RI, 30–800 pmol/L) and < 1 mU/L (RI, 3.3–4.1 mU/L), respectively. Her urinary free cortisol level was 17.0 nmol/L (RI, 0.4–5.2 nmol/L) and urinary cortisone was 23.0 nmol/L (RI, 1.9–14.9 nmol/L), conferring a urinary cortisol:cortisone ratio of 0.7 (RI, 0.3–0.5). Serum corticosterone and 11‐deoxycorticosterone levels were 3.95 nmol/L (RI, 3.75–23.67 nmol/L) and < 0.05 nmol/L (RI, < 0.57 nmol/L), respectively.
The clinical picture was thought to be due to excess liquorice intake, resulting in apparent mineralocorticoid excess (AME). The herbal tea consumption was ceased immediately. In view of severe hypokalaemia, she received intravenous and oral potassium; however, ongoing hypokalaemia was noted. She was commenced on spironolactone 75 mg daily and her potassium levels gradually normalised. Owing to persistent hypertension, she transiently required nifedipine, which was ceased a few days later.
On follow‐up after 18 days, her symptoms had resolved and her biochemistry improved, with aldosterone and renin levels of 240 pmol/L and 2 mU/L, respectively. Her blood pressure normalised and remained so following withdrawal of spironolactone.
Discussion
The syndrome of AME, which has features similar to primary aldosteronism, is characterised by hypokalaemia, hypertension, metabolic alkalosis and low plasma renin. However, plasma aldosterone levels are low in AME as opposed to the elevated levels that occur in primary aldosteronism. AME can either be congenital, due to a deficiency in 11‐β‐hydroxysteroid dehydrogenase type 2 (11‐β‐HSD2), or acquired as a result of exogenous causes such as liquorice ingestion.
Liquorice is present in a variety of confectionery, teas, chewing gums, cough mixtures, complementary medicines and alcoholic drinks. It is frequently prescribed by naturopaths for many medical conditions. Liquorice tea‐induced AME has been reported in the literature previously.1,2
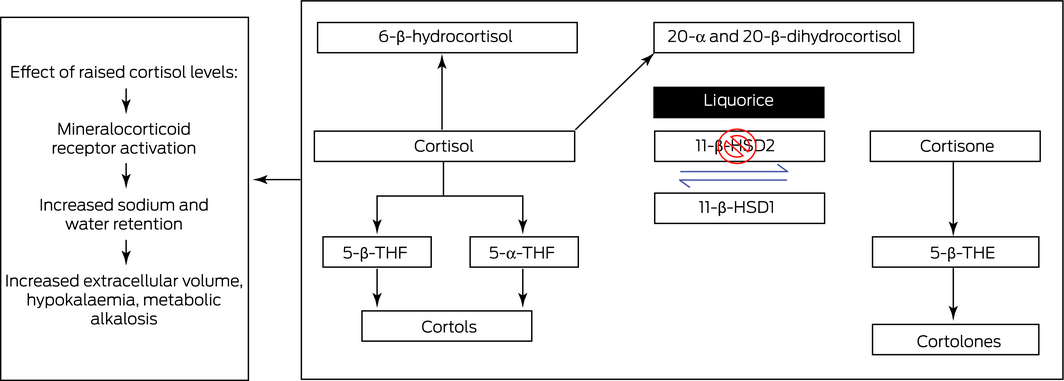
The mechanism of liquorice‐induced AME is related to the glycyrrhizic acid contained in liquorice. Once absorbed in the intestine, glycyrrhizic acid is converted to the pharmacologically active compound glycyrrhetinic acid, which inhibits 11‐β‐HSD2, which converts active glucocorticoid cortisol to locally inactive cortisone (Box 2).3 The relative increase in cortisol activates mineralocorticoid receptors in the kidney, causing an increase in sodium and water retention and potassium wasting, and a subsequent increase in extra‐cellular volume, hypokalaemia and metabolic alkalosis.4
The glycrryhizic acid content varies between products, with a typical liquorice pipe containing 4.6 mg, while a serve of liquorice tea contains 20 mg.5,6 The onset and severity of the syndrome depends on the amount of liquorice consumed, duration of consumption and individual susceptibility. The factors that play a role in an individual's susceptibility to the effects of glycyrrhizic acid remain unknown.7,8 Doses as low as 100 mg have been known to cause AME syndromes.8
Other differential diagnoses worth considering include genetically linked AME caused by a deficiency in 11‐β‐HSD2, and endocrinopathies such as Cushing syndrome, ectopic corticotropin syndrome and Liddle syndrome.4,9 The presence of normal cortisol and adrenocorticotropic hormone levels excludes Cushing syndrome, and the subsequent improvement in renin and aldosterone levels effectively excludes other endocrinopathies.
The urinary free cortisol to urinary cortisone ratio is a valuable diagnostic indicator. In congenital AME caused by 11‐β‐HSD2 deficiency, the levels of cortisone are very low; the urinary cortisol to cortisone ratio is usually between 5 and 18.10 In ectopic adrenocorticotropic hormone production, patients have a similarly increased cortisol to cortisone ratio; however, in contrast to 11‐β‐HSD2 deficiency, both urinary cortisol and cortisone levels are elevated.11 In our patient, the modestly elevated urinary free cortisol to urinary cortisone ratio of 0.74 is suggestive of chronic liquorice ingestion, as the urinary free cortisone was only slightly decreased.
Liquorice is increasingly used in a variety of food products as well as herbal medicines. Given its increasing use, the presence of hypokalaemia, oedema and hypertension should prompt practitioners to consider the diagnosis of liquorice‐induced AME.
Lessons from practice
- Chronic ingestion of liquorice can result in the syndrome of mineralocorticoid excess, characterised by hypokalaemia, hypertension, metabolic alkalosis, and low plasma renin and aldosterone levels.
- Liquorice‐induced apparent mineralocorticoid excess is reversible following withdrawal of the offending agent, but a brief course of a mineralocorticoid antagonist may be needed.
- The urinary free cortisol to urinary cortisone ratio can help differentiate liquorice‐induced apparent mineralocorticoid excess from other differential diagnoses including 11‐β‐hydroxysteroid dehydrogenase type 2 deficiency, Cushing syndrome, ectopic corticotropin syndrome and Liddle syndrome.
Box 1 – Biochemistry results
Follow‐up after admission | |||||||||||||||
Results (reference interval) |
Admission |
Discharge |
18 days |
26 days | |||||||||||
Sodium (133–146 mmol/L) |
145 |
141 |
142 |
142 |
|||||||||||
Potassium (3.6–5.4 mmol/L) |
2.5 |
5.2 |
4.4 |
4.6 |
|||||||||||
Creatinine (45–90 umol/L) |
55 |
64 |
60 |
55 |
|||||||||||
eGFR (mL/min/1.732) |
> 90 |
> 90 |
> 90 |
> 90 |
|||||||||||
Renin (3.3–4.1 mU/L) |
< 1 |
2 |
|||||||||||||
Aldosterone (30–800 pmol/L) |
< 27 |
240 |
|||||||||||||
Aldosterone:renin ratio (< 70) |
Not calculable |
120 |
|||||||||||||
Cortisol (100–540 nmol/L) |
190 |
452 |
|||||||||||||
ACTH (0–12 pmol/L) |
8.5 |
5.6 |
|||||||||||||
Urinary free cortisol (0.4–5.2 nmol/L) |
17.0 |
||||||||||||||
Urinary cortisone (1.9–14.9 nmol/L) |
23.0 |
||||||||||||||
Urinary cortisol:cortisone ratio (0.30–0.50) |
0.74 |
||||||||||||||
Serum corticosterone (3.75–23.67 nmol/L) |
3.95 |
||||||||||||||
11‐deoxycorticosterone (< 0.57 nmol/L) |
< 0.05 |
||||||||||||||
ACTH = adrenocorticotropic hormone; eGFR = estimated glomerular filtration rate. | |||||||||||||||
Competing interests
No relevant disclosures.
References
- Gallacher SD, Tsokolas G, DImitropoulos I. Licorice‐induced apparent mineralocorticoid excess presenting in the emergency department. Clin Med (Lond) 2017; 17: 1–43.
- Lin SH, yang SS, Chau T, Halperin ML. An unusual cause of hypokalaemic paralysis: chronic licorice ingestion. Am J Med Sci 2003; 325: 153–156.
- van Uum SH, Lenders JW, Hermus AR. Cortisol, 11 beta‐hydroxysteroid dehydrogenases, and hypertension. Semin Vasc Med 2004; 4: 121–128.
- Palermo M, Quinkler M Stewart PM. Apparent mineralocorticoid excess syndrome: an overview. Arq Bras Endocrinol Metabol 2004; 48: 687–696.
- Stormer FC, Reistad R, Alexander J. Glycyrrhizic acid in liquorice–evaluation of health hazard. Food Chem Toxicol 1993; 31: 303–312.
- Spinks EA, Fenwick GR. The determination of glycyrrhizin in selected UK liquorice products. Food Addit Contam 1990; 7: 769–778.
- Walker BR, Edwards C. Licorice‐induced hypertension and syndromes of apparent mineralocorticoid excess. Endocrinol Metab Clin North Am 1994; 23: 359–377.
- Olukoga A, Donaldson D. Liquorice and its health implications. J R Soc Promot Health 2000; 120: 83–89.
- Armanini D, Calò L, Semplicini A. Pseudohyperaldosteronism: pathogenetic mechanisms. Crit Rev Clin Lab Sci 2003; 40: 295–335.
- Palermo M, Delitala G, Mantero F, et al. Congenital deficiency of 11beta‐hydroxysteroid dehydrogenase (apparent mineralocorticoid excess syndrome): diagnostic value of urinary free cortisol and cortisone. J Endocrinol Invest 2001; 24: 17–23.
- Palermo M, Shackleton CH, Mantero F, Stewart PM. Urinary free cortisone and the assessment of 11 beta‐hydroxysteroid dehydrogenase activity in man. Clin Endocrinol 1996; 45: 605–611.
Provenance: Not commissioned; externally peer reviewed.