




Many Australians living in rural and remote areas of Australia need to travel hundreds of kilometres for health care service, or to wait for health service providers, such as the Royal Flying Doctor Service (RFDS), to visit them. The levels of acute and subacute hospital services in rural and remote areas are reported to be inadequate,1 as is, to a lesser extent, access to aged care services.2 The need to travel long distances is a major barrier for people in remote locations, particularly older people, seeking health care.
National data on health care for older Australians are available,3 but we do not have a clear picture of the specific problems of older people living in rural and remote areas who require aeromedical retrieval for treatment. We therefore briefly describe in this report the health characteristics of older Australians who have been retrieved at least once by the RFDS and the primary health care services accessible to them within 60 minutes by road.
We undertook a cross‐sectional review of prospectively collected routine patient data for older Australians (Indigenous patients aged 55 years or more; non‐Indigenous patients aged 65 years or more4) retrieved by the RFDS from anywhere in Australia between 1 July 2014 and 31 June 2017. To assess population health service coverage, we entered the locations of available health services (source: Health Direct; https://about.healthdirect.gov.au) into the RFDS Service Planning and Operational Tool (SPOT), and then overlaid 2016 census data provided by the Australian Bureau of Statistics. The study was approved by the Australian Capital Territory Health Service Human Research Ethics Committee (reference, 2018/QA/00184).
During 2014–2017, the RFDS conducted 21 877 aeromedical retrievals of older patients (30.7% of 71 230 RFDS aeromedical retrievals); 13 673 patients (62.5%) were retrieved once, 2045 (9.4%) twice. Of 18 252 retrievals of non‐Indigenous patients (83.4% of retrievals), 11 023 were of male (60%) and 7228 of female patients (40%). The most frequent reasons for retrieval were acute myocardial infarction (827 retrievals, 4.5%), fracture of the femur (620, 3.4%), convalescence (332, 1.8%), angina pectoris (213, 1.2%), and hypertensive renal disease (175, 1.0%). Of the 3625 retrievals of Indigenous Australians (16.6% of retrievals), 1671 were of male (46%) and 1953 of female patients (54%). The most frequent reasons for retrieval were acute myocardial infarction (82 retrievals, 2.3%), pneumonia (60, 1.7%), fracture of the femur (40, 1.1%), sepsis (35, 1.0%), and stroke (26, 0.7%) (Box 1).
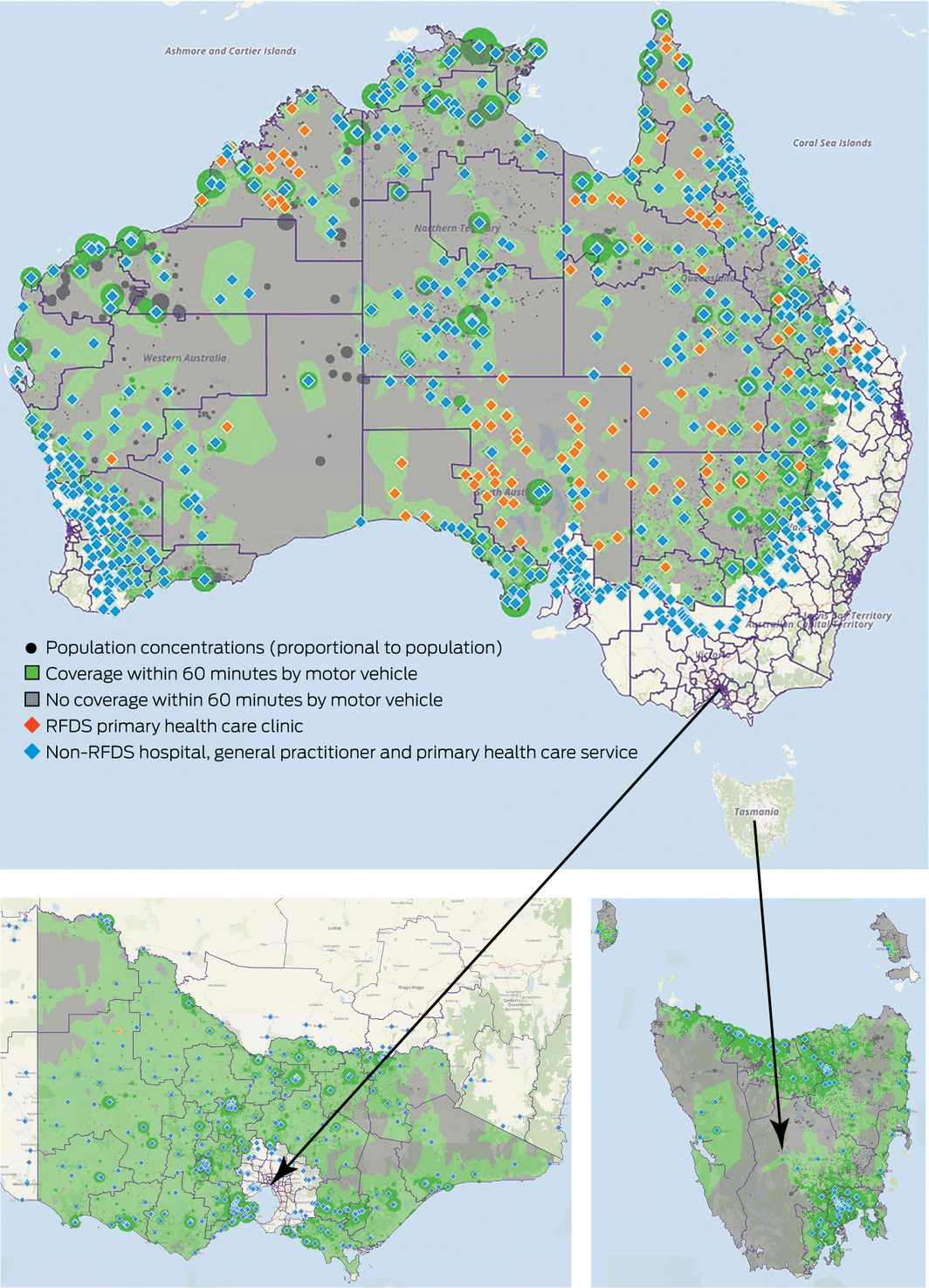
Many rural and remote areas do not have easy access to hospitals or primary health care (Box 2). A large proportion of people in rural and remote regions need to drive for more than 60 minutes to reach health services, including hospitals, emergency departments, primary health care, and rehabilitation and management services.
The RFDS is essential for providing health care in rural and remote areas. Many older patients have no other access to care because of the small populations of their communities, the distances to larger population centres, and shortfalls in local health care provision. This is a major problem, given that the most frequent reason for retrieval was myocardial infarction, which requires early treatment and extensive long term management and rehabilitation.5
Box 1 – International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD‐10) diagnoses for older patients transported by the Royal Flying Doctor Service, 2014–15 to 2016–17
|
ICD‐10 code diagnosis |
Males |
Females |
Total |
||||||||||||
|
|
|||||||||||||||
|
Non‐Indigenous patients: retrievals |
11 024 |
7228 |
18 252 |
||||||||||||
|
I21 Acute myocardial infarction |
555 (3.0%) |
272 (1.5%) |
827 (4.5%) |
||||||||||||
|
S72 Fracture of femur |
230 (1.3%) |
390 (2.1%) |
620 (3.4%) |
||||||||||||
|
Z54 Convalescence |
202 (1.1%) |
130 (0.7%) |
332 (1.8%) |
||||||||||||
|
I20 Angina pectoris |
147 (0.8%) |
66 (0.4%) |
213 (1.2%) |
||||||||||||
|
I12 Hypertensive renal disease |
120 (0.7%) |
55 (0.3%) |
175 (1.0%) |
||||||||||||
|
K92 Other diseases of digestive system |
102 (0.6%) |
53 (0.3%) |
155 (0.8%) |
||||||||||||
|
K56 Paralytic ileus and intestinal obstruction without hernia |
87 (0.5%) |
66 (0.4%) |
153 (0.8%) |
||||||||||||
|
I64 Stroke, not specified as haemorrhage or infarction |
98 (0.5%) |
55 (0.3%) |
153 (0.8%) |
||||||||||||
|
I48 Atrial fibrillation and flutter |
89 (0.5%) |
44 (0.2%) |
133 (0.7%) |
||||||||||||
|
I49 Cardiac arrhythmias |
101 (0.6%) |
27 (0.1%) |
128 (0.7%) |
||||||||||||
|
J18 Pneumonia |
74 (0.4%) |
51 (0.3%) |
125 (0.7%) |
||||||||||||
|
I50 Heart failure |
71 (0.4%) |
46 (0.3%) |
117 (0.6%) |
||||||||||||
|
A41 Sepsis |
80 (0.4%) |
46 (0.3%) |
126 (0.7%) |
||||||||||||
|
R10 Abdominal and pelvic pain |
56 (0.3%) |
42 (0.2%) |
98 (0.5%) |
||||||||||||
|
I45 Conduction disorders |
66 (0.4%) |
31 (0.2%) |
97 (0.5%) |
||||||||||||
|
All other diagnoses |
8946 (49.0%) |
5854 (32.1%) |
14 800 (81.1%) |
||||||||||||
|
Indigenous patients: retrievals |
1671 |
1953 |
3625 |
||||||||||||
|
I21 Acute myocardial infarction |
40 (1.1%) |
42 (1.2%) |
82 (2.3%) |
||||||||||||
|
J18 Pneumonia |
27 (0.7%) |
33 (0.9%) |
60 (1.7%) |
||||||||||||
|
S72 Fracture of femur |
9 (0.2%) |
31 (0.9%) |
40 (1.1%) |
||||||||||||
|
A41 Sepsis |
19 (0.5%) |
16 (0.4%) |
35 (1.0%) |
||||||||||||
|
I64 Stroke, not specified as haemorrhage or infarction |
9 (0.2%) |
17 (0.5%) |
26 (0.7%) |
||||||||||||
|
J44 Chronic obstructive pulmonary disease |
13 (0.4%) |
8 (0.2%) |
21 (0.6%) |
||||||||||||
|
I20 Angina pectoris |
12 (0.3%) |
9 (0.2%) |
21 (0.6%) |
||||||||||||
|
I50 Heart failure |
7 (0.2%) |
10 (0.3%) |
17 (0.5%) |
||||||||||||
|
R10 Abdominal and pelvic pain |
9 (0.2%) |
8 (0.2%) |
17 (0.5%) |
||||||||||||
|
Z54 Convalescence |
7 (0.2%) |
9 (0.2%) |
16 (0.4%) |
||||||||||||
|
J81 Pulmonary oedema |
4 (0.1%) |
11 (0.3%) |
15 (0.4%) |
||||||||||||
|
N17 Acute renal failure |
6 (0.2%) |
7 (0.2%) |
13 (0.4%) |
||||||||||||
|
I24 Other acute ischaemic heart diseases |
5 (0.1%) |
7 (0.2%) |
12 (0.3%) |
||||||||||||
|
K92 Other diseases of digestive system |
7 (0.2%) |
5 (0.1%) |
12 (0.3%) |
||||||||||||
|
K56 Paralytic ileus and intestinal obstruction without hernia |
8 (0.2%) |
4 (0.1%) |
12 (0.3%) |
||||||||||||
|
All other diagnoses |
1489 (41.1%) |
1736 (47.9%) |
3226 (89.0%) |
||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Received 7 February 2019, accepted 19 June 2019
- 1. Davis J, Morgans A, Stewart J. Developing an Australian health and aged care research agenda: a systematic review of evidence at the subacute interface. Aust Health Rev 2016; 40: 420–427.
- 2. van Gaans D, Dent E. Issues of accessibility to health services by older Australians: a review. Public Health Rev 2018; 39: 20.
- 3. Australian Institute of Health and Welfare. Older Australia at a glance (AGE 87). Canberra: AIHW, 2018. https://www.aihw.gov.au/reports/older-people/older-australia-at-a-glance (viewed June 2019).
- 4. Gardiner FW, Gale L, Bishop L, Laverty M. Healthy ageing in rural and remote Australia: challenges and gaps in service provision to overcome. Canberra: The Royal Flying Doctor Service of Australia, 2018. https://www.flyingdoctor.org.au/assets/documents/RN069_Healthy_Ageing_Report_D3.pdf (viewed June 2019).
- 5. Cui X, Zhou X, Ma LL, et al. A nurse‐lead structured education program improves self‐management skills and reduces hospital readmissions in patients with chronic heart failure: a randomized and controlled trial. Rural Remote Health 2019; 19: 5270.
No relevant disclosures.