





Medical education
Lessons from practice
Volume 210 - Issue 10
Surface antigen negative hepatitis B infection: the importance of screening before B cell‐depleting therapy
Authors: Sanjivan Mudaliar, Ken Liu and Simone I Strasser
Med J Aust 2019; 210 (10): 442-443.e1. || doi: 10.5694/mja2.50165
Published online: 3 June 2019
Published online: 3 June 2019
Evidence suggests that appropriate hepatitis B virus (HBV) screening before B cell-depleting therapy is frequently not performed
Clinical record
A 68‐year old man who was a migrant from Greece underwent 6 months of treatment with the anti‐CD20 B cell‐depleting agent obinutuzumab and chlorambucil for chronic lymphocytic leukaemia. Over this period, his widespread lymphadenopathy regressed, and his lymphocyte count normalised from a peak of 29 × 109/L (reference interval [RI], 4–10× 109/L). He was negative for hepatitis B virus (HBV) surface antigen (HBsAg) on HBV screening performed before treatment. HBV core antibody (anti‐HBc) was not tested. Routine monitoring during and after treatment demonstrated a progressive elevation of liver enzymes from a normal baseline (Box). When the alanine aminotransferase (ALT) level reached 420 U/L (RI, 5–55 U/L) at 6 months after treatment completion, a full serological panel along with HBV DNA revealed anti‐HBc and HBV e antigen (HBeAg) positivity, with a HBV DNA level of 26 700 000 IU/mL (7.4 log10), but persistently negative HBsAg despite this clear reactivation flare. Testing for hepatitis C virus revealed no evidence of infection. There were no features of hepatic decompensation. He was immediately commenced on entecavir 0.5 mg daily. However, because the effect of entecavir on stopping active liver inflammation by suppressing viral replication is not immediate, his ALT level continued to climb to a peak of 1488 U/L after 4 weeks of treatment. At this time, he underwent HBeAg seroconversion, becoming HBeAg negative with progressive reduction in HBV DNA and normalisation of ALT level over the next 4 months. Of particular note, he remained persistently HBsAg negative throughout follow‐up. Subsequent testing revealed multiple mutations in the gene encoding HBsAg protein, which prevented epitope binding by commercially available HBsAg assays.
Discussion
About 1–10% of Australians have current (HBsAg positive) or previous (HBsAg negative and anti‐HBc positive) HBV infection, respectively.1 Potentially fatal reactivation of chronic hepatitis B following chemotherapy or immunosuppressive therapy is widely recognised in many clinical scenarios.
The new Australian consensus statement recommends screening all patients undergoing therapy for haematological malignancy with both HBsAg and anti‐HBc, and commencing antiviral prophylaxis in HBsAg seropositive individuals.1 However, reactivation has also been reported in HBsAg negative and anti‐HBc positive patients,1 presumed to be related to the presence of ongoing low level intrahepatic viral replication. Evidence suggesting the risk of reactivation in these HBsAg negative and anti‐HBc positive patients exceeds 10% when they receive B cell‐depleting, B cell active or anti‐CD20 agents; therapy for acute leukaemia and high grade lymphoma; or haematopoietic cell transplant.2 Prophylaxis is also recommended in this setting,1 but screening practices remain inconsistent and antivirals are underprescribed.3 A recent South Australian statewide cohort study found that, of 438 patients who were prescribed rituximab over a 12‐month period, only 52.3% of patients received appropriate HBsAg and anti‐HBc screening.4 HBsAg screening alone was performed in 27.2% of patients, and 19.6% of patients did not receive pre‐treatment screening at all.4
In our case, the patient likely had occult HBV infection that was missed by screening only with an HBsAg assay. Occult HBV infection is defined as the presence of detectable HBV DNA in the serum or the liver, despite an undetectable HBsAg. Its prevalence is rare in Australia (reported as 0.69% in a high risk Australian population),5 but can reach 45–51% in HBV endemic populations.6 The reason for variation in reported prevalence rates is unclear, but may reflect differences in testing rates, assay sensitivity, or sample sizes or biological differences in populations. In our patient, the negative HBsAg result in the pre‐treatment screening was due to mutations in the gene encoding HBsAg and provided false reassurance that his hepatitis was unlikely caused by HBV in the 6‐month period during which his ALT level, and presumably HBV DNA, gradually rose (Box). Of note, a similar flare may have occurred in this situation if the patient had previous resolved (HBsAg negative and anti‐HBc positive) HBV infection, although in this situation the HBsAg usually reverts to positive. Therefore, HBsAg alone is inadequate to determine HBV reactivation risk in patients receiving B cell‐depleting therapy or haematopoietic cell transplant.
Australian cohort data4 suggest failure to follow testing recommendations before B cell‐depleting therapy is common. While screening with HBsAg and anti‐HBc will detect occult HBV infection, as in the case presented, more importantly, it will also detect the far more common situation of resolved HBV infection that is also associated with significant risk of reactivation. Antiviral prophylaxis in these patients by using nucleoside or nucleotide analogues with a high barrier to resistance (entecavir or tenofovir) significantly reduces the risk of a reactivation flare. Prophylaxis should be continued for 18–24 months after cessation of B cell‐depleting therapy or haematopoietic cell transplant, and for 6–12 months after other cancer therapies, unless the patient otherwise fulfils the criteria for hepatitis B treatment.1 This case is a reminder of the need for thorough screening and prophylaxis for HBV in patients receiving intensive chemotherapy or immunosuppressive therapy.
Lessons from practice
- Evidence suggests that appropriate hepatitis B virus (HBV) screening before B cell‐depleting therapy is frequently not performed.
- At a minimum, screening tests should include HBV surface antigen (HBsAg) and HBV core antibody (anti‐HBc); testing for HBsAg alone is inadequate.
- There is at least a 10% risk of a reactivation flare in HBsAg negative and anti‐HBc positive (resolved infection) patients who undergo B cell‐depleting therapy.
- Antiviral prophylaxis in HBsAg positive and in HBsAg negative and anti‐HBc positive patients receiving B cell‐depleting therapy reduces the risk of life‐threatening HBV reactivation.
Box – Laboratory values of patient throughout course of hepatitis B virus (HBV) reactivation after obinutuzumab*
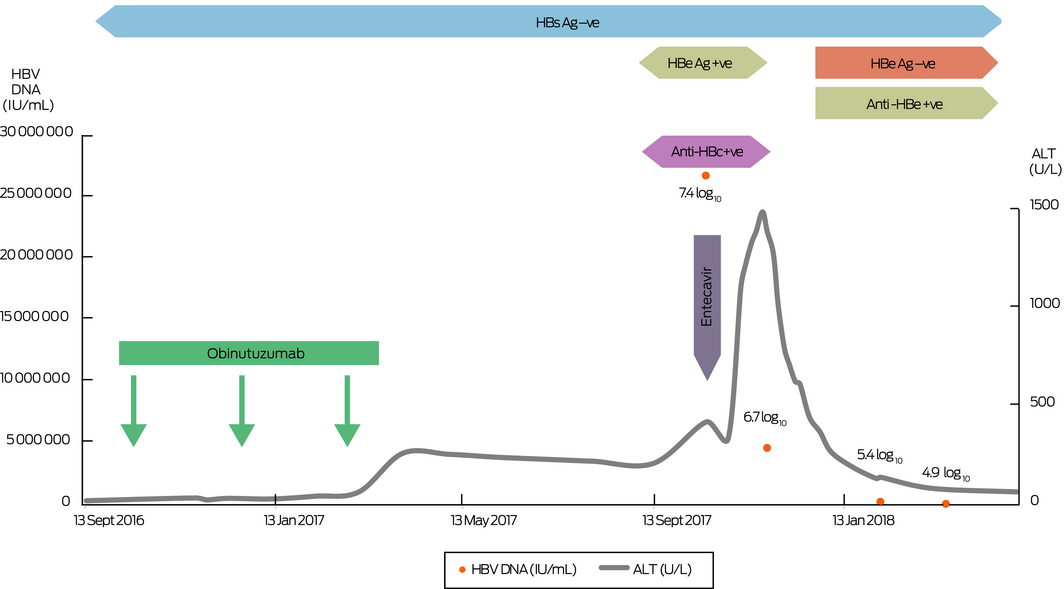
ALT = alanine aminotransferase; anti‐HBc = HBV core antibody; HBeAg = HBV e antigen; HBsAg = HBV surface antigen. +ve = positive; −ve = negative. *The course of ALT, HBV DNA level and serology in a 68‐year‐old man who experienced HBsAg negative HBV reactivation causing asymptomatic hepatitis following B cell‐depleting therapy. ◆
Competing interests
No relevant disclosures.
References
- Doyle J, Raggatt M, Slavin M, et al. Hepatitis B management during immunosuppression for haematological and solid organ malignancies: an Australian consensus statement. Med J Aust 2019; 210: 000–000.
- Perrillo RP, Gish R, Falck‐Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015; 148: 221–44.
- Wi CI, Loo NM, Larson JJ, et al. Low level of hepatitis B virus screening among patients receiving chemotherapy. Clin Gastroenterol Hepatol 2015; 13: 970–975.
- Sal H, Shaikh A, Teh K, et al. Hepatitis B screening before ritixumab therapy: a multicentre South Australian study of adherence. Intern Med J 2018; 48: 936–943.
- Martinez MC, Kok CC, Baleriola C, et al. Investigation of occult hepatitis B virus infection in anti‐HBc positive patients from a liver clinic. PLoS One 2015 Mar 12; 10: e0117275.
- Raimondo G, Pollicino T, Cacciola I, et al. Occult hepatitis B virus infection. J Hepatol 2007; 46: 160–170.
Provenance: Not commissioned; externally peer reviewed.