




The known Decompensated cirrhosis is characterised by recurrent hospital admissions and is associated high morbidity, mortality, and cost. The role of chronic disease management, the standard of care for chronic diseases such as congestive heart failure, is not well studied in patients with decompensated cirrhosis.
The new Patients with decompensated cirrhosis managed in a coordinated care model, a chronic liver failure program supervised by hepatologists, had fewer liver-related emergency re-admissions and better survival than patients managed with standard care.
The implications Multicentre randomised controlled trials that examine the efficacy of our chronic liver failure program are warranted.
Cirrhosis is a chronic liver disease, and is associated with multiple complications and repeated hospital admissions for as many as 50% of patients in whom it progresses to hepatic decompensation.1,2 In Australia, an estimated 6.2 million people have some form of chronic liver disease,3 and the annual number of deaths it caused increased by 31% between 2006 and 2015.4 The frequent re-admissions that are characteristic of decompensated cirrhosis contribute to the substantial financial cost of managing liver disease;3 an Australian study found that the incidence of liver-related emergency admissions within 30 days of initial discharge among patients with decompensated cirrhosis with ascites was 42%.5 In a prospective multicentre study in the United States, 50% of hospitalised patients with decompensated cirrhosis were re-admitted within 90 days;2 in a retrospective study, the 30-day re-admission rate was 37%, with 22% of re-admissions classified as preventable.6
A coordinated system of care for patients with cardiac failure — chronic disease management — has been associated with significant cost savings and reduced rates of heart failure-related admissions and mortality.7-9 In a randomised pilot trial, our group found that patients with decompensated cirrhosis treated in a chronic liver failure program based on chronic disease management principles were more likely to attend clinic and surveillance (endoscopy and radiology) appointments.10 Since 2010, the chronic liver failure program has been an integral part of care for patients with decompensated cirrhosis at our hospital.
As re-admission rates and survival are key quality indicators when evaluating chronic disease management,11 we compared these parameters for our institution and its coordinated care model with those of another major hospital in our health region that provides standard care for patients with decompensated cirrhosis.
Methods
Study design
The study was a retrospective observational cohort study in two major hospitals in an Australian capital city with different models of care for managing patients with decompensated cirrhosis.
Models of care
Unit 1 (U1) is a 593-bed general hospital with an intensive care unit, an accident and emergency unit, and inpatient gastroenterology and hepatology units; it also houses the centre for the state liver transplantation service. A coordinated care model is practised in U1; patients with decompensated cirrhosis are managed in a liver unit staffed by gastroenterologists with a special interest in hepatology, and post-discharge care is coordinated in a chronic liver failure program, a chronic disease management intervention we have previously described.10 The multifaceted intervention encompasses four chronic disease management domains: delivery system redesign, decision support, self-management support, and clinical information systems. Its key aims are to improve adherence to evidence-based care and to enhance post-discharge monitoring of patients by providing protocol-based checklists and care plans for post-discharge care, post-discharge phone calls, home visits, self-management support with enhanced patient and carer education, patient action plans for dealing with complications (ascites, encephalopathy), access to day care therapeutic large volume paracentesis, and a rapid care pathway for patients whose condition is deteriorating. Two experienced hepatology nurses (0.6 full-time positions) support the program in close consultation with the hepatologists. Patients are provided with office hours contact numbers for the nurses and are encouraged to call when they feel unwell or have worsening abdominal distension, altered sensorium, or gastrointestinal bleeding.
Unit 2 (U2) is a 680-bed general hospital with an intensive care unit, an accident and emergency unit, and an inpatient gastroenterology and hepatology unit. Patients with decompensated cirrhosis are managed in a general gastroenterology or general medical ward. Patients attend follow-up clinics as advised at the time of discharge, without organised follow-up by nurses. No elective paracentesis is arranged, and nurses do not liaise between specialists and patients. Patients present to the emergency department if they are unwell.
Patients in both the units had the same access to liver transplantation services when referred to the liver transplantation unit at U1.
Inclusion and exclusion criteria
Patients admitted to each hospital with a diagnosis of a decompensated cirrhosis-related event during October 2013 – October 2014 were identified on the basis of International Classification of Diseases (ICD-10) codes for cirrhosis and its complications as primary and secondary diagnoses. Patients (U1, 62; U2, 68) were excluded if they died during the initial admission or after referral to palliative care, were lost to follow-up, or were admitted for an elective procedure without decompensated cirrhosis. As our study involved voluntary access to the public health system, some patients had been admitted to both U1 and U2; seven patients with equal numbers of admissions to each unit were therefore excluded from our study, as were four patients admitted to other public hospitals after their initial admission to either U1 or U2. Patients were followed until the end of October 2016, liver transplantation, loss to follow-up, or death.
Classification of admission types
We assessed electronic medical records of eligible patients for hospital re-admissions during the study period. Hospitalisations were classified as liver-related emergency, liver-related elective, non-liver-related emergency, and non-liver-related elective admissions. Liver-related emergency admission was defined as an unplanned hospitalisation following presentation to the emergency department with variceal bleed, ascites, hepatic encephalopathy, sepsis, cellulitis, pneumonia, urosepsis, hepato-renal syndrome, hepatic hydrothorax, electrolyte disturbances, or hepato-pulmonary syndrome. Liver-related elective admissions included planned admissions without presentation to the emergency department, such as abdominal or thoracic paracentesis, radiological procedures for hepatocellular carcinoma, liver transplantation workup, and same day admission for deterioration detected in the outpatient clinic. Non-liver-related emergency admissions included those for chest pain, abdominal pain unrelated to liver disease, fractures, trauma, and alcohol intoxication or substance misuse without decompensated cirrhosis-related problems. When patients were admitted for non-liver-related reasons, such as cataract surgery, they were classified as non-liver-related elective admissions. The presence of significant medical comorbid conditions was assessed with the Charlson comorbidity index.
Statistical analysis
All analyses were conducted in SPSS Statistics for Windows 23 (IBM) or Stata 14.1 (StataCorp). The mean incidence rates (with 95% confidence intervals [CIs]) of liver-related and non-liver-related emergency and elective admissions were calculated with Poisson exact methods. Admission rates for the two units were compared and incident rate ratios (IRRs) calculated by negative binomial regression, adjusted for age, sex, aetiology, comorbid conditions (Charlson index), and Model for End-Stage Liver Disease (MELD) score.12
Characteristics of the patients at the two units were compared in independent t tests (normally distributed continuous variables), Mann–Whitney tests (non-normally distributed continuous variables), or χ2 tests (categorical variables).
Differences in estimated transplantation-free survival rates between U1 and U2 were analysed with Kaplan–Meier methods and log-rank tests (univariate analysis), and by Cox regression (multivariate analysis). Variables in the univariate analysis for which P < 0.15 were included in the multivariate model; they were deemed significant predictors of transplantation-free survival if P < 0.05 in the multivariate model.
Ethics approval
Ethics approval was obtained from the Human Research Ethics Committees of U2 (reference, HREC/17/RAH/83); as the study was a quality improvement initiative, it was exempt from formal ethics committee review at U1.
Results
A total of 123 patients (U1, 69; U2, 54) were eligible for inclusion; the median follow-up time was 530 days (range, 21–1105 days). There were no statistically significant differences between the two units other than the higher mean Charlson comorbidity score for U1 patients: 6.0 (standard deviation [SD], 2.3) v 5.2 (SD, 1.9; P = 0.043) (Box 1).
Liver-related emergency admissions
The frequency of complications of cirrhosis identified at the initial and the first liver-related emergency admissions are summarised in Box 2. The overall mean rate of liver-related emergency admissions during the study period was 1.31 per person per year (95% CI, 1.15–1.48 per person per year), consisting of 241 admissions over 184 person-years. For U2, the mean rate was 1.55 per person per year (95% CI, 1.28–1.85 per person per year), comprising 119 admissions over 77 person-years; for U1, it was 1.14 per person per year (95% CI, 0.95–1.36 per person per year), comprising 122 admissions over 107 person-years. The unadjusted IRR (U1 v U2) was 0.58 (95% CI, 0.32–1.05; P = 0.07); after adjusting for age, sex, baseline MELD score, alcohol-related aetiology, and comorbid conditions, the IRR was 0.52 (95% CI, 0.28–0.98; P = 0.042). The overall median time to first re-admission was 67 days (range, 3–620 days); for U1 it was 74 days (range, 3–488 days), for U2, 51 days (range, 3–620 days; P = 0.80).
A total of 80 patients (65%) had at least one liver-related emergency admission, 62 (50%) had two or more, and 41 (33%) had three or more (U1, 18 [26%]; U2, 22 [41%]; P = 0.08). Nine patients in U1 (13%) and 13 in U2 (24%) were re-admitted for a liver-related emergency within 30 days of discharge (P = 0.10); 29 patients in U1 (41%) and 23 in U2 (47%) were re-admitted within 90 days (P = 0.57).
All admissions
The incidence rates of admissions to the two hospitals are compared in Box 3. Liver-related elective admissions were higher for U1 than for U2 (IRR, 4.60; 95% CI, 1.92–11.0; P < 0.001).
Liver transplantation
Two patients referred from U2 successfully underwent liver transplantation. Of the 12 patients from U1 listed for transplantation, nine had successful liver transplantations, one was delisted, and three died while on the waiting list.
Survival analysis
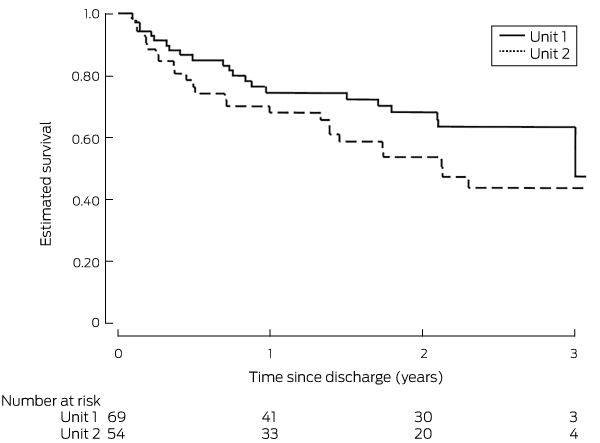
In the univariate survival analysis, the influence of MELD score, occurrence of any liver-related emergency admission, liver-related emergency admissions within 30 and 90 days of discharge, non-alcohol-related aetiology, and the presence of significant comorbid conditions (as measured by Charlson comorbidity index score), age, and sex were each significant (P < 0.15). Survival for patients in U1 and U2 in the univariate analysis is shown in Box 4. In the multivariate analysis (including significant univariate factors), unit (U2 v U1: hazard ratio [HR], 2.54; 95% CI, 1.26–5.09; P = 0.009), liver-related emergency admission within 90 days of discharge (HR, 3.60; 95% CI, 1.87–6.92; P < 0.001), and Charlson comorbidity index score (per point: HR, 1.27; 95% CI, 1.05–1.54; P = 0.014) were significant predictors of reduced survival (Box 5). The adjusted rate of transplantation-free survival at 3 years (according to the estimated survivor function following Cox regression) was significantly higher for U1 (67.7% v 37.2% in U2; P = 0.009).
Discussion
In this study, we compared the long term effects of managing decompensated cirrhosis with a coordinated care model, including key quality indicators such as numbers of liver-related emergency admissions and transplantation-free survival, with those of standard care as offered by another large hospital in the same metropolitan health region. The incidence of liver-related emergency admissions was significantly lower and transplantation-free survival higher for patients treated in the coordinated care model. Lower rates of emergency admissions, some of which may be high value admissions (ie, clinically appropriate), can be detrimental to the patient and lead to higher mortality,13 but, after adjusting for age, sex, baseline MELD score, alcohol-related aetiology, and the presence of comorbid conditions, mortality was lower among patients receiving coordinated care. These patients also had more elective re-admissions, reflecting the successful delivery of planned care, and probably contributing to the reduced incidence of liver-related emergency admissions.
We assessed the contributions of factors at the level of the patient, hospital facilities, and care model to the differences in outcomes between hospitals. Despite the higher mean Charlson index comorbidity score for patients in U1, their outcomes were superior to those of patients in U2. Liver disease severity, as assessed by MELD scores, was similar for the patients of the two hospitals. U1 and U2 were similar with regard to features considered advantageous,14 including having high volumes of patients with cirrhosis, emergency and intensive care departments, academic hospital status, and advanced endoscopic and radiological facilities.
The two hospitals differed distinctly in one key area: their model of care. While we cannot exclude that other, unmeasured factors contributed to the differences in rates of liver-related emergency admissions and survival, it is probable that the coordinated care model was the crucial factor. It is difficult to identify the specific aspect of the multifaceted care model most likely to have contributed to its positive effects, but the dedicated inpatient liver unit, staffed by gastroenterologists with a special interest and experience in hepatology and liver transplantation, may have been important, as specialist care has been associated with reduced mortality among patients with decompensated cirrhosis.15 The presence of the state liver transplantation unit at U1 may have influenced outcomes, as transplantation centres are associated with lower in-hospital mortality among patients with cirrhosis.14 However, patients in U1 and U2 had equal access to the liver transplant facility.
In addition to the differences in inpatient care, the dedicated post-discharge monitoring program, led by specialist hepatology nurses, was probably also critical for the better outcomes for patients of U1. Better post-discharge monitoring, greater self-management by patients, and adherence to evidence-based care plans may have led to potential emergency admissions becoming elective hospitalisations. The lower rates of liver-related emergency admissions and mortality for patients of U1 are consistent with reports that close attention to quality indicators when managing ascites, including early paracentesis and initiation of diuretic therapy, reduces 30-day re-admission rates and 90-day mortality.16
Ascites was the most common reason for hospitalisation, both at baseline and during follow-up. The frequency of ascites as a reason for re-admission was lower than that for the initial admission among patients of U1, but not those of U2. It seems likely that the specific components of the coordinated care model regarding ascites — education about reducing dietary salt, weekly monitoring of electrolytes and weight, nurse-facilitated elective paracentesis — played a role in reducing ascites-related emergency admissions.
Limitations
Limitations include the retrospective design of the study, the small numbers of patients, and the possibility that unmeasured factors influenced the main outcomes. These limitations may have led us to overestimate the benefit of the coordinated care model. Nevertheless, our findings are important, given the high prevalence and cost of managing patients with decompensated cirrhosis in Australia.
Conclusion
Our investigation highlights the differences in key quality indicators, such as mortality and incidence of emergency admissions, for patients with cirrhosis of similar severity who are managed in equivalent health care settings but with different models of care. Verifying the clinical efficacy and cost-effectiveness of this model of care in a large multicentre prospective, randomised controlled trial should be a research priority.
Box 1 – Baseline clinical and demographic characteristics of eligible patients in Units 1 and 2
|
Characteristic |
U1 |
U2 |
P |
||||||||||||
|
|
|||||||||||||||
|
Number of patients |
69 |
54 |
|
||||||||||||
|
Age (years), mean (SD) |
59.2 (10.4) |
56.0 (10.2) |
0.08 |
||||||||||||
|
Sex (men) |
47 (68%) |
36 (67%) |
0.86 |
||||||||||||
|
Aetiology: non-alcohol-related |
23 (33%) |
10 (18%) |
0.07 |
||||||||||||
|
Diabetes |
29 (42%) |
14 (26%) |
0.06 |
||||||||||||
|
Charlson comorbidity index score, mean (SD) |
6.0 (2.3) |
5.2 (1.9) |
0.043 |
||||||||||||
|
MELD score, mean (SD) |
17.4 (6.3) |
16.8 (5.8) |
0.61 |
||||||||||||
|
Follow-up (days), median (range) |
622 (32–1086) |
508 (21–1105) |
0.35 |
||||||||||||
|
|
|||||||||||||||
|
MELD = Model for End-Stage Liver Disease; SD = standard deviation. |
|||||||||||||||
Box 2 – Indications for initial hospital admission and first liver-related emergency re-admission
|
Indication* |
Initial admission |
First re-admission |
|||||||||||||
|
Total |
U1 |
U2 |
Total |
U1 |
U2 |
||||||||||
|
|
|||||||||||||||
|
Number of patients |
123 |
69 |
54 |
80 |
45 |
35 |
|||||||||
|
Ascites-related |
70 (57%) |
45 (65%) |
25 (46%) |
38 (48%) |
22 (49%) |
16 (47%) |
|||||||||
|
Hepatic encephalopathy |
33 (27%) |
17 (25%) |
16 (30%) |
32 (40%) |
19 (42%) |
13 (37%) |
|||||||||
|
Variceal bleeding |
33 (27%) |
11 (16%) |
22 (41%) |
14 (18%) |
4 (9%) |
10 (29%) |
|||||||||
|
Sepsis-related† |
21 (17%) |
10 (14%) |
11 (20%) |
18 (22%) |
14 (31%) |
4 (11%) |
|||||||||
|
Miscellaneous‡ |
8 (7%) |
1 (1%) |
7 (6%) |
9 (11%) |
4 (5%) |
5 (6%) |
|||||||||
|
|
|||||||||||||||
|
* Most patients had more than one complication. † Including spontaneous bacterial peritonitis or cellulitis, pneumonia, urosepsis, bacteraemia, septic arthritis. ‡ Including portal hypertensive gastropathy-related bleeding, portal vein thrombosis, ulcer bleeding causing decompensation, alcoholic hepatitis, bleeding caused by thrombocytopaenia. |
|||||||||||||||
Box 3 – Rates of liver- and non-liver-related emergency and elective admissions to Units 1 and 2
|
Admission category |
Mean admission rate (95% CI) |
Incidence rate ratio (95% CI) |
|||||||||||||
|
U1 |
U2 |
Unadjusted |
P |
Adjusted* |
P |
||||||||||
|
|
|||||||||||||||
|
Total person-years |
107 |
77 |
|
|
|
|
|||||||||
|
Liver-related emergency |
1.14 (0.95–1.36) |
1.55 (1.28–1.85) |
0.58 (0.32–1.05) |
0.07 |
0.52 (0.28–0.98) |
0.042 |
|||||||||
|
Non-liver-related emergency |
0.53 (0.40–0.69) |
0.51 (0. 37–0.70) |
0.95 (0.51–1.81) |
0.89 |
0.72 (0.38–1.38) |
0.33 |
|||||||||
|
Liver-related elective |
3.48 (3.14–3.85) |
0.50 (0. 36–0.69) |
4.60 (1.92–11.0) |
< 0.001 |
4.42 (1.69–11.6) |
0.002 |
|||||||||
|
Non-liver-related elective |
0.22 (0.14–0.33) |
0.08 (0.03–0.17) |
2.62 (0.94–7.34) |
0.07 |
1.39 (0.47–4.10) |
0.55 |
|||||||||
|
|
|||||||||||||||
|
* Adjusted for age, sex, aetiology, comorbid conditions (Charlson index), and Model for End-Stage Liver Disease (MELD) score. |
|||||||||||||||
Box 5 – Cox regression survival analysis model*
|
Factor |
Hazard ratio (95% CI) |
P |
|||||||||||||
|
|
|||||||||||||||
|
Sex (women v men) |
0.76 (0.38–1.59) |
0.48 |
|||||||||||||
|
Alcohol-related aetiology |
0.83 (0.37–1.89) |
0.67 |
|||||||||||||
|
Age (per year) |
1.02 (0.99–1.07) |
0.17 |
|||||||||||||
|
Baseline MELD (per point) |
1.04 (0.99–1.10) |
0.07 |
|||||||||||||
|
Charlson comorbidity index score (per point) |
1.27 (1.05–1.54) |
0.014 |
|||||||||||||
|
Unit (U2 v U1) |
2.54 (1.26–5.09) |
0.009 |
|||||||||||||
|
Liver-related emergency re-admission within 90 days of discharge |
3.60 (1.87–6.92) |
< 0.001 |
|||||||||||||
|
|
|||||||||||||||
|
MELD = Model for End-Stage Liver Disease. * Full data available for 108 patients. (U1, 68; U2, 40). |
|||||||||||||||
Received 27 November 2017, accepted 3 May 2018
- Jeyamani Ramachandran1,2
- Monowar Hossain1
- Chris Hrycek1
- Edmund Tse3
- Kate R Muller1,2
- Richard J Woodman4
- Billingsley Kaambwa5
- Alan J Wigg1,2
- 1 Flinders Medical Centre, Adelaide, SA
- 2 College of Medicine and Public Health, Flinders University, Adelaide, SA
- 3 Royal Adelaide Hospital, Adelaide, SA
- 4 Flinders Centre for Epidemiology and Biostatistics, Flinders University, Adelaide, SA
- 5 Flinders University, Adelaide, SA
No relevant disclosures.
- 1. Ge PS, Runyon BA. Treatment of patients with cirrhosis. N Engl J Med 2016; 375: 2104-2105.
- 2. Bajaj JS, Reddy KR, Tandon P, et al; North American Consortium for the Study of End-Stage Liver Disease. The 3-month readmission rate remains unacceptably high in a large North American cohort of patients with cirrhosis. Hepatology 2016; 64: 200-208.
- 3. Deloitte Access Economics. The economic cost and health burden of liver diseases in Australia. Melbourne: The Gastroenterological Society of Australia/Australian Liver Association, 2013. http://www.gesa.org.au/resources/economic-cost-and-health-burden-of-liver-disease-in-australia (viewed Sept 2017).
- 4. Australian Bureau of Statistics. 3303.0. Causes of death, Australia, 2015. Sept 2016. http://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/3303.0Main+Features100012015?OpenDocument (viewed Sept 2017).
- 5. Fagan KJ, Zhao EY, Horsfall LU, et al. Burden of decompensated cirrhosis and ascites on hospital services in a tertiary care facility: time for change? Intern Med J 2014; 44: 865-872.
- 6. Volk ML, Tocco RS, Bazick J, et al. Hospital readmissions among patients with decompensated cirrhosis. Am J Gastroenterol 2012; 107: 247-252.
- 7. McAlister FA, Stewart S, Ferrua S, McMurray JJJV. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol 2004; 44: 810-819.
- 8. Gonseth J, Guallar-Castillón P, Banegas JR, Rodríguez-Artalejo F. The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: a systematic review and meta-analysis of published reports. Eur Heart J 2004; 25: 1570-1595.
- 9. Roccaforte R, Demers C, Baldassarre F, et al. Effectiveness of comprehensive disease management programmes in improving clinical outcomes in heart failure patients: a meta-analysis. Eur J Heart Fail 2005; 7: 1133-1144.
- 10. Wigg AJ, McCormick R, Wundke R, Woodman RJ. Efficacy of a chronic disease management model for patients with chronic liver failure. Clin Gastroenterol Hepatol 2013; 11: 850-858, e1-4.
- 11. Benbassat J, Taragin MI. The effect of clinical interventions on hospital readmissions: a meta-review of published meta-analyses. Isr J Health Policy Res 2013; 2: 1.
- 12. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology 2001; 33: 464.
- 13. Fan VS, Gaziano JM, Lew R, et al. A comprehensive care management program to prevent chronic obstructive pulmonary disease hospitalizations: a randomized, controlled trial. Ann Intern Med 2012; 156: 673-683.
- 14. Mathur AK, Chakrabarti AK, Mellinger JL, et al. Hospital resource intensity and cirrhosis mortality in United States. World J Gastroenterol 2017; 23: 1857-1865.
- 15. Bini EJ, Weinshel EH, Generoso R, et al. Impact of gastroenterology consultation on the outcomes of patients admitted to the hospital with decompensated cirrhosis. Hepatology 2001; 34: 1089-1095.
- 16. Le S, Spelman T, Chong CP, et al. Could adherence to quality of care indicators for hospitalized patients with cirrhosis-related ascites improve clinical outcomes? Am J Gastroenterol 2016; 111: 87-92.
Abstract
Objectives: To compare the incidence of liver-related emergency admissions and survival of patients after hospitalisation for decompensated cirrhosis at two major hospitals, one applying a coordinated chronic disease management model (U1), the other standard care (U2); to examine predictors of mortality for these patients.
Design: Retrospective observational cohort study.
Setting: Two major tertiary hospitals in an Australian capital city.
Participants: Patients admitted with a diagnosis of decompensated cirrhosis during October 2013 – October 2014, identified on the basis of International Classification of Diseases (ICD-10) codes.
Main outcome measures: Incident rates of liver-related emergency admissions; survival (to 3 years).
Results: Sixty-nine patients from U1 and 54 from U2 were eligible for inclusion; the median follow-up time was 530 days (range, 21–1105 days). The incidence of liver-related emergency admissions was lower for U1 (mean, 1.14 admissions per person-year; 95% CI, 0.95–1.36) than for U2 (mean, 1.55 admissions per person-year; 95% CI, 1.28–1.85; adjusted incidence rate ratio [U1 v U2], 0.52; 95% CI, 0.28–0.98; P = 0.042). The adjusted probabilities of transplantation-free survival at 3 years were 67.7% (U1) and 37.2% (U2) (P = 0.009). Independent predictors of reduced transplantation-free free survival were Charlson comorbidity index score (per point: hazard ratio [HR], 1.27; 95% CI, 1.05–1.54, P = 0.014), liver-related emergency admissions within 90 days of discharge (HR, 3.60; 95% CI, 1.87–6.92; P < 0.001), and unit (U2 v U1: HR, 2.54, 95% CI, 1.26–5.09; P = 0.009).
Conclusions: A coordinated care model for managing patients with decompensated cirrhosis was associated with improved survival and fewer liver-related emergency admissions than standard care.