





Volume 209 - Issue 4
Management of bronchiectasis in adults
Authors: Simone K Visser, Peter Bye and Lucy Morgan
Med J Aust 2018; 209 (4): 177-183. || doi: 10.5694/mja17.01195
Published online: 20 August 2018
Published online: 20 August 2018
Bronchiectasis is gaining recognition as an important chronic lung disease of increasing prevalence
Summary
- Once neglected in research and underappreciated in practice, there is renewed interest in bronchiectasis unrelated to cystic fibrosis.
- Bronchiectasis is a chronic lung disease characterised by chronic cough, sputum production and recurrent pulmonary exacerbations. It is diagnosed radiologically on high resolution computed tomography chest scan by bronchial dilatation (wider than the accompanying artery).
- The causes of bronchiectasis are diverse and include previous respiratory tract infections, chronic obstructive pulmonary disease, asthma, immunodeficiency and connective tissue diseases. A large proportion of cases are idiopathic, reflecting our incomplete understanding of disease pathogenesis.
- Progress in the evidence base is reflected in the 2017 European management guidelines and the 2015 update to the Australian guidelines.
- Effective airway clearance remains the cornerstone of bronchiectasis management. This should be personalised and reviewed regularly by a respiratory physiotherapist.
- There is now robust evidence for the long term use of oral macrolide antibiotics in selected patients to reduce exacerbation frequency.
- The routine use of long term inhaled corticosteroids and/or long-acting bronchodilators should be avoided, unless concomitant chronic obstructive pulmonary disease or asthma exists.
- The evidence for nebulised agents including hypertonic saline, mannitol and antibiotics is evolving; however, access is challenging outside tertiary clinics, and nebulising equipment is required.
- Smokers should be supported to quit. All patients should receive influenza and pneumococcal vaccination. Patients with impaired exercise capacity should attend pulmonary rehabilitation.
- There is an important minority of patients for whom aetiology-specific treatment exists.
- The prevalence of bronchiectasis is increasing worldwide; however, the burden of disease within Australia is not well defined. To this end, the Australian Bronchiectasis Registry began recruitment in 2016 and is interoperable with the European and United States bronchiectasis registries to enable collaborative research.
- The recent addition of a bronchiectasis diagnosis-related group to the Australian Refined Diagnostic Related Group classification system will allow definition of the disease burden within the Australian hospital system.
Bronchiectasis is a chronic lung disease of diverse aetiology, characterised by a clinical syndrome of chronic cough, sputum production and recurrent pulmonary exacerbations. It is defined radiologically by abnormal bronchial dilatation.1
The reported prevalence of bronchiectasis continues to increase worldwide,2-4 with recent prevalence estimates in the United Kingdom of 566 per 100 000 women and 485 per 100 000 men.3 Females, the elderly,2-4 and Indigenous populations5 are more frequently affected. Notably, Indigenous children in Australia’s Northern Territory have an extremely high disease prevalence of 14.7 per 1000 children;6 however, no large study examining the prevalence of bronchiectasis in Australia has been conducted. The economic burden of bronchiectasis is significant; a recent study conducted in New Zealand reported an annual hospitalisation cost of NZD$5.34 million.7 Quality of life impairment in patients with bronchiectasis is equivalent to the impairment seen in patients with severe chronic obstructive pulmonary disease (COPD).1
Historically, bronchiectasis not due to cystic fibrosis has been neglected in research. This is reflected in the absence of licensed medications for bronchiectasis across Australia, the United States and Europe. Encouragingly, within the past 5 years, research has gained worldwide momentum with the establishment of bronchiectasis registries in Europe and the United States. On a national level, the Australian Bronchiectasis Registry began recruitment in 2016 and a bronchiectasis-specific code was added to the Australian Refined Diagnostic Related Group classification system in 2016.8 Moreover, where there was an absence of high quality evidence to guide bronchiectasis management, in recent years Australian and New Zealand researchers have contributed significantly to the now robust evidence in support of maintenance macrolide antibiotics to reduce pulmonary exacerbations.9,10 Developments in the evidence base are reflected in the 2017 European Respiratory Society bronchiectasis management guidelines1 and in the recently updated Australian guidelines.11
This article reviews the management of bronchiectasis in adults, which is timely given the evolving evidence base and the increasing prevalence and recognition of the disease in clinical practice. Citations were derived from PubMed, Scopus and the Cochrane Library using the terms “non-cystic fibrosis bronchiectasis” or “bronchiectasis” and “treatment” or “management” or “antibiotic” or “inhaled” or “nebul*” or “physiotherapy”, as well as from searching the bibliographies of recent review articles and guidelines.
Pathogenesis and diagnosis
Radiological bronchiectasis is diagnosed using a high resolution computed tomography chest scan when the bronchial diameter exceeds that of the adjacent vessel (broncho-arterial ratio > 1).12 However, the broncho-arterial ratio may be affected by age, and studies indicate that 20–40% of the healthy population over 65 years of age have abnormally high ratios.13,14 Hence, the term “clinically significant bronchiectasis” is used when the radiological diagnosis accompanies the syndrome of cough, sputum, and recurrent respiratory infection. Further recommendations refer to clinically significant bronchiectasis. In addition to airway dilation, a high resolution computed tomography chest scan may show mucus plugging and thickened airway walls, and is important to document disease extent and location, and guide airway clearance manoeuvres.
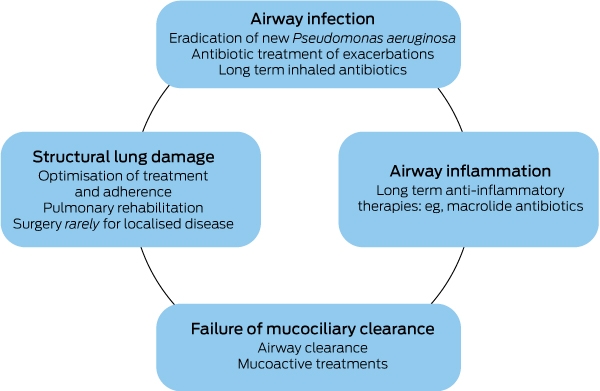
A diverse range of conditions (Box 1) lead to the common pathological endpoint of bronchiectasis,15 through a cycle of impaired mucus clearance, bacterial colonisation, inflammation, and structural damage occurring in the airways (Box 2).1 On a finer mechanistic level, disease pathogenesis remains incompletely understood; an interplay between genetic susceptibility, immune dysregulation, increased airway neutrophils and neutrophil elastase, and bacterial infection are implicated.16 Idiopathic bronchiectasis is probably relatively rare, but tests of the many subtle abnormalities of immune function are not robust or readily accessible,16 nor is patient recall of past infective illnesses necessarily reliable.
It is important to identify those minority of cases for which specific treatment exists. Box 3 describes the minimum tests recommended for all adult bronchiectasis patients.1,11 Abnormal test results should prompt specialist referral for further investigation and management (Box 4).1,11,12,17,18
General recommendations
The objectives of treatment in bronchiectasis are to improve symptoms and quality of life, reduce exacerbations, and limit disease progression.1 Treatable causes must be identified and specifically addressed (Box 3 and Box 4), however even when a treatable cause is present, the following recommendations apply.
The majority of patients with bronchiectasis produce sputum on a daily basis.19 Augmentation of sputum clearance is critical and should be the cornerstone of daily treatment. Airway clearance makes physiological sense, is safe, inexpensive, and improves quality of life and sputum expectoration.20 All patients should be referred to a specialised respiratory physiotherapist, who can personalise an airway clearance regimen.17 This may include a combination of aerobic exercise, active cycle of breathing, positive expiratory pressure devices and postural drainage.1,11
Smokers should be supported to quit and all patients should receive influenza and pneumococcal vaccination. Patients with impaired exercise capacity should attend pulmonary rehabilitation.11 Surgery is considered rarely for those with localised disease and frequent exacerbations despite optimal management.1 Selected patients with severe disease may be suitable for lung transplant, although there is a paucity of outcome data.12 Excellent resources for patients and clinicians are available from the Thoracic Society of Australia and New Zealand and Lung Foundation Australia.21,22
Many patients may be maintained with an exercise and airway clearance regimen. However, the following medications may be required and prescribed in collaboration with a respiratory physician (Box 5). The indications for specialist review are outlined in Box 6.12
Antibiotics
Patients with bronchiectasis may require antibiotics in four main situations:1,11,23
-
to treat pulmonary exacerbations;
-
to attempt eradication of new Pseudomonas aeruginosa in sputum;
-
as long term treatment to reduce exacerbation frequency and symptoms; or
-
to treat non-tuberculous mycobacterial pulmonary disease.
The choice of antibiotic should be guided by the goal of therapy, clinical severity, airway microorganisms and their antibiotic susceptibility (obtained from sputum or bronchoscopy samples), prior antibiotic response, allergies and drug interactions.1,11 High quality evidence to guide antibiotic approach in bronchiectasis is limited. At the time of writing, there are at least four Cochrane Reviews underway investigating aspects of antibiotic use in bronchiectasis.24-27
It should be noted that bronchiectasis patients often have positive sputum culture results.28 With the exception of an exacerbation and/or new isolation of P. aeruginosa, positive cultures alone do not mandate antibiotics.1
Treatment of exacerbations
An exacerbation is defined as deterioration from baseline in three or more of the following symptoms for at least 48 hours, and which a clinician decides requires a change in treatment:29 cough, sputum volume and/or consistency, sputum purulence, breathlessness and/or exercise tolerance, fatigue and/or malaise, and haemoptysis.
The severity of an exacerbation is judged on clinical grounds (eg, significantly deranged vital signs compared with the patient’s baseline would indicate a severe exacerbation).
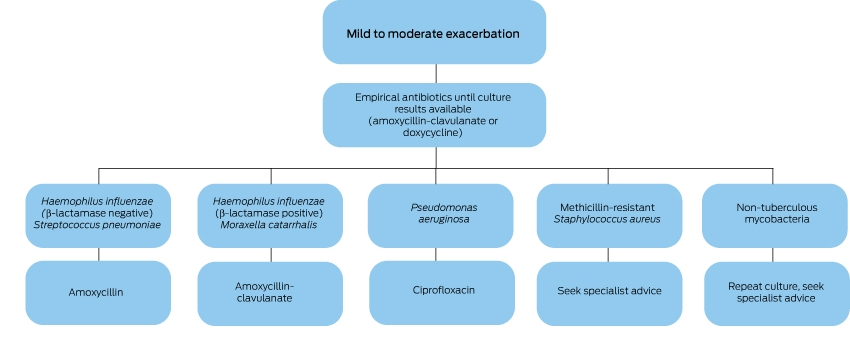
At the onset of an exacerbation, a sputum sample should be sent for microscopy, culture and sensitivity. If available, previous airway culture and sensitivity results should guide antibiotic choice, otherwise empirical therapy is commenced while culture results are awaited. Box 7 and Box 8 outline a suggested approach to empirical therapy.17,30
Based on low quality evidence and consensus opinion, the recommended duration of antibiotics for an exacerbation is 14 days.1 In practice, antibiotics for 7–14 days are usually prescribed, depending on the clinical situation. Intravenous antibiotics for severe exacerbations are usually continued for at least 5 days, and often followed by oral antibiotics for a total duration of 10–14 days.11
Eradication of Pseudomonas aeruginosa
New isolation of P. aeruginosa in sputum should prompt consideration of antibiotics for eradication,1,11,12,31 as this pathogen confers a worse prognosis. The optimal eradication regime has not been determined, however common practice is to prescribe two weeks of oral ciprofloxacin and then repeat the sputum culture. If the culture remains positive for P. aeruginosa, treatment may be escalated to intravenous or inhaled antibiotics.1,11,12,31 Specialist advice is recommended. There is currently no evidence to support eradication of other organisms.1
Long term antibiotics to reduce exacerbation frequency and symptoms
Under specialist supervision, long term antibiotics (inhaled and/or oral) should be considered in patients who continue to have recurrent or severe exacerbations despite optimal management (good airway clearance regimes, underlying causes treated). Long term macrolide antibiotics currently have the highest level of evidence for reducing exacerbations.1
Long term inhaled antibiotics
Inhaled antibiotics (eg, gentamicin, tobramycin, colistin, ciprofloxacin) may be trialled in selected patients with bacterial colonisation and recurrent exacerbations. Inhaled antibiotics have theoretical advantages in the ability to deliver a high concentration of drug to the airway while markedly reducing systemic absorption and toxicity. There is clear evidence that inhaled antibiotics reduce sputum bacterial load,32-34 and reduced bacterial load has been shown to reduce airway inflammation.35
The use of inhaled antibiotics is challenging however due to the difficulty in accessing these medications for the (non-cystic fibrosis) bronchiectasis population and the incidence of bronchospasm which approximates 10–30% with nebulised aminoglycosides.1,11 Moreover, large trials demonstrating significant improvement in hard clinical endpoints (such as reduced exacerbation frequency) are limited.
Inhaled tobramycin solution was shown in a small phase 2 trial to reduce bacterial density after 28 days treatment, at the expense of increased cough, dyspnoea, wheeze and chest pain.36 A phase 3 trial of tobramycin inhalation solution for bronchiectasis is currently recruiting (NCT02657473), as is a phase 1 trial of dry powder tobramycin (NCT02712983).
A small randomised controlled trial (RCT) of gentamicin nebulised for 12 months demonstrated reduced bacterial density and reduced exacerbations. 22% of participants experienced wheeze, which did not result in withdrawal from the trial, and no ototoxicity or nephrotoxicity was reported.37
A phase 3 trial of colistin nebulised for 6 months showed a trend towards increased time to first exacerbation; this finding was statistically significant when the adherent subgroup was analysed. This trial also demonstrated improvements in quality of life.38 A second phase 3 trial of inhaled colistin is currently recruiting (NCT03093974).
Recent phase 3 trials of aztreonam inhaled for 28 days did not meet their primary endpoint of improved quality of life, and dropouts mainly due to cough and dyspnoea were significantly elevated in the treatment groups.39
Large phase 3 studies of inhaled ciprofloxacin are now complete. RESPIRE 1 and 240,41 (dry powder ciprofloxacin, on-off treatment cycles for 48 weeks, in patients with positive sputum culture at screening for one of seven predefined organisms) and ORBIT 3 and 4 (liposomal ciprofloxacin, on-off treatment cycles for 48 weeks, in patients with chronic P. aeruginosa)42 both used time to first exacerbation and frequency of exacerbations as primary endpoints. RESPIRE 1 and 2 showed trends towards reduced exacerbations, which only met significance in one of two treatment arms (14 days on/off) of the RESPIRE 1 trial. Similarly, ORBIT 4 met the primary endpoints but ORBIT 3 did not. In the ORBIT pooled analysis there was a significant reduction in exacerbation frequency. These large trials showed that inhaled ciprofloxacin is well tolerated (40-42). Promotion of ciprofloxacin resistance with long term use is of concern, particularly as ciprofloxacin is the only oral treatment available for exacerbations in P. aeruginosa colonised patients. The RESPIRE trials reported an increased percentage of sputum pathogens with elevated minimal inhibitory concentrations in the treatment arms compared with placebo arms.40,41 Additional studies will be required to determine ciprofloxacin efficacy and monitor resistance.
The evidence base for long term inhaled antibiotics is emerging. In specialist practice, inhaled antibiotics are prescribed “month on, month off” for carefully chosen patients with recurrent exacerbations, usually with P. aeruginosa colonisation, who tolerate inhaled antibiotics and show a clinical improvement on therapy.31
Long term oral antibiotics
Long term oral antibiotics can also be considered for patients with recurrent exacerbations who are otherwise optimally managed, but should not be prescribed routinely.1,11
Macrolides exert immunomodulatory and antibiotic effects. They have been shown to reduce exacerbation frequency in three well-conducted RCTs of 6–12 months duration. The BAT43 and EMBRACE10 trials used azithromycin, whereas the Australian BLESS trial used erythromycin.9 Reduced exacerbation frequency has been confirmed in meta-analyses which included smaller studies, alternative macrolides, and paediatric data.44-46 Patients with P. aeruginosa colonisation may derive greater benefit;9 however, airway colonisation with P. aeruginosa or other airway pathogens is not a prerequisite for consideration of macrolide treatment.
Patient selection is important. Under specialist supervision, a therapeutic trial (12–24 months) of maintenance macrolide therapy should be considered in patients with recurrent and/or severe exacerbations who are otherwise optimally managed. Prior to macrolide commencement, non-tuberculous mycobacteria (NTM) should be excluded, and a normal QT interval corrected for heart rate on electrocardiogram should be confirmed.1,11
The benefits of macrolides must be weighed against the risk of resistance and side effects. Reduced exacerbation frequency comes at the expense of an increase in macrolide resistance organisms in the oropharynx9 and sputum;43 however, the significance of this is unclear at present. Macrolide monotherapy may induce resistance in NTM, which has implications as macrolides are often used in combination therapy for NTM pulmonary disease. Further, macrolides prolong the QT interval and may increase adverse cardiac events,47 although this was not observed in the three small bronchiectasis RCTs.9,10,43 Macrolide therapy has been associated with hearing decrements in the COPD population; discussion with patients and clinical monitoring is prudent; baseline audiometry could be considered.47
Other long term oral antibiotics (eg, doxycycline or amoxicillin) can be considered in cases of macrolide contraindication or intolerance;1 however, the evidence for alternative antibiotic classes is limited to small historical trials showing reduced sputum purulence and less days off work with oxytetracycline48 and amoxicillin.49,50
Treatment of non-tuberculous mycobacterial pulmonary disease
NTM are ubiquitous environmental organisms that are emerging as increasingly prevalent lung pathogens that can cause or complicate bronchiectasis.23 Progressive inflammatory lung disease (NTM pulmonary disease) must be distinguished from asymptomatic infection or transiently positive sputum cultures. Treatment of NTM pulmonary disease relies on prolonged multidrug regimens with significant side effects and variable success. A decision to treat is not undertaken lightly. Readers are referred to recent NTM pulmonary disease guidelines.23
Mucoactive agents
Nebulised saline and mannitol increase hydration of the airway surface, alter mucus rheology and increase mucociliary clearance.51 They may be trialled in patients who have a substantial sputum burden, difficulty expectorating sputum, poor quality of life and/or frequent exacerbations despite standard airway clearance techniques.1,11
It is unclear whether hypertonic saline is superior to isotonic saline in the non-cystic fibrosis bronchiectasis population. The evidence is limited to two small, randomised trials with conflicting results. In 28 patients undertaking a single-blind crossover study of nebulised 7% saline and 0.9% saline for 3 months, Kellett and colleagues found improvements in lung function, quality of life and health care utilisation when participants were receiving hypertonic saline.52 However, in a 12-month double-blind randomised trial comparing 0.9% and 6% nebulised saline in 40 patients, Nicolson and colleagues found that both groups showed improvements in exacerbations, quality of life, lung function and sputum colonisation compared with baseline.53
The randomised double-blind placebo-controlled trials of inhaled dry powder mannitol failed to meet their primary endpoints. In the first, inhaled mannitol for 3 months in 343 patients failed to show a difference in quality of life, and demonstrated a reduction in 24-hour sputum weight in the placebo group which was associated with increased antibiotic use in this group.54 The subsequent trial in 461 patients over 12 months also failed to meet its primary endpoint of reduced exacerbations, but did show an increased time to first exacerbation.55
Notably, recombinant human deoxyribonuclease is contraindicated in bronchiectasis without cystic fibrosis. The large multicentre randomised double-blind, placebo-controlled trial of deoxyribonuclease in non-cystic fibrosis bronchiectasis found a deleterious effect on lung function and exacerbation frequency.56
Bronchodilators and corticosteroids
Short-acting bronchodilators are recommended before inhalation of mucoactive agents and/or inhaled antibiotics, particularly in those with symptomatic bronchoconstriction, to improve drug tolerability and deposition.1,11
The widespread use of inhaled long-acting bronchodilators (LABD) and corticosteroids in bronchiectasis is driven by extrapolation from the asthma and COPD literature and is not supported by any high level evidence. A Cochrane review of inhaled corticosteroid (ICS) use in bronchiectasis concluded that the evidence did not support routine use of ICS and posed a risk of adverse effects.57 Evidence for long term use of inhaled long-acting β-agonists (LABA) in stable bronchiectasis is limited to one unblinded trial in 40 subjects, comparing combined ICS/LABA (budesonide 640 μg and formoterol 18 μg) with high dose ICS (budesonide 1600 μg).58 Patients who received ICS/LABA had less dyspnoea and more cough-free days after 3 months of treatment than those on ICS alone, with no difference in lung function or exacerbations. However, these findings were potentially the result of a harmful control group; the ICS group predictably had increased adverse events, which were incompletely described. The evidence for long-acting muscarinic receptor antagonists (LAMA) in the bronchiectasis population is extremely limited. A recent RCT of tioptropium versus placebo in 90 stable bronchiectasis patients with airflow obstruction reported very modest improvements in forced expiratory volume in 1 second, but did not report improvements in exacerbation rates, symptoms, or quality of life.59
The routine use of LABD and/or ICS for bronchiectasis is not recommended. However, in the case of concomitant reactive airways disease or COPD, ICS and/or LABD should be prescribed as appropriate for these conditions. Guidelines also make a weak recommendation based on low quality evidence that LABD can be trialled in very breathless bronchiectasis patients on an individual basis.1,11
Conclusion
Bronchiectasis is gaining recognition as an important chronic lung disease of increasing prevalence, which places a significant burden on the health care system and the individual. The goals of therapy are to improve symptoms, reduce exacerbations and limit progression of disease, and the mainstay of treatment is effective airway clearance. The evidence base for the management of this once neglected disease is evolving. The evidence for macrolide antibiotics is robust, and recent European and Australian management guidelines recommend the use of prophylactic macrolides to reduce exacerbation frequency in selected patients with recurrent and/or severe exacerbations. The ecological consequences of long term macrolide use with respect to bacterial resistance have yet to be fully investigated. Data from the Australian Bronchiectasis Registry and the addition of an Australian Refined Diagnostic Related Group bronchiectasis code will provide insight into the burden of disease and patterns of care in Australia.
Box 1 – Causes of bronchiectasis in adults15
- Idiopathic, ∼ 40%
- Post-infective, ∼ 30%
- Immunodeficiency, ∼ 5%*
- Chronic obstructive pulmonary disease, ∼ 5%*
- Connective tissue disease, ∼ 4%*
- Allergic bronchopulmonary aspergillosis, ∼ 3%*
- Primary ciliary dyskinesia, ∼ 2%*
- Asthma, ∼ 1%*
- Non-tuberculous mycobacteria*
- Infrequent causes, < 1%: inflammatory bowel disease, gastro-oesophageal reflux/aspiration, α-1 antitrypsin deficiency, diffuse panbronchiolitis, pink disease, yellow nail syndrome, bronchial obstruction, congenital malformations, inhaled foreign body
Box 3 – Diagnostic approach to adult bronchiectasis: minimum tests1,11
|
Investigation* |
Significance |
Comment |
|||||||||||||
|
|
|||||||||||||||
|
Full blood count and differential white cell count |
Neutropenia/lymphopenia/lymphocytosis may suggest immune deficiency; eosinophilia suggests asthma or ABPA |
Requires further investigation and specific management |
|||||||||||||
|
Serum total IgE, specific IgG and IgE to Aspergillus (± Aspergillus skin prick testing) |
Total IgE > 1000 IU/mL and positive Aspergillus serology is consistent with ABPA |
ABPA treated with oral steroids ± antifungals |
|||||||||||||
|
Serum IgG, IgM, IgA |
Low immunoglobulin levels suggest a primary (eg, CVID) or secondary immunodeficiency state |
Further history and testing required. May warrant immunoglobulin replacement† |
|||||||||||||
|
Sputum MCS and AFB |
To document microbiology and direct future antibiotic treatment |
Multiple samples recommended at baseline, ≥ 12 monthly thereafter, or at onset of exacerbation |
|||||||||||||
|
Spirometry |
To document baseline lung function and allow monitoring |
An acute fall in spirometry (in association with other features) suggests pulmonary exacerbation |
|||||||||||||
|
Oximetry |
To document baseline oxygen saturations, allow monitoring, guide further tests (eg arterial blood gas) and guide treatment |
See for indications for domiciliary oxygen |
|||||||||||||
|
|
|||||||||||||||
|
ABPA = allergic bronchopulmonary aspergillosis; AFB = acid-fast bacilli; CVID = common variable immune deficiency; HRCT = high resolution computed tomography; MCS = microscopy culture and sensitivity; * Recommended for all patients with confirmed bronchiectasis on HRCT chest scan. † See https://www.criteria.blood.gov.au for eligibility criteria for intravenous Ig. |
|||||||||||||||
Box 4 – Diagnostic approach to adult bronchiectasis: discretionary tests1,11,12,17,18
|
Investigation |
Possible indications |
Comment |
|||||||||||||
|
|
|||||||||||||||
|
Arterial blood gas |
If peripheral oxygen saturations low or severe disease |
Consider domiciliary oxygen if PaO2 ≤ 55 mmHg while stable in non-smoking patients or 56–59 mmHg with evidence of hypoxic organ damage;18 selected patients may require non-invasive ventilation |
|||||||||||||
|
Bronchoscopy |
If foreign body or airway abnormality suspected, or to obtain specimens for culture |
|
|||||||||||||
|
Autoimmune/connective tissue disease blood panel |
If suggestive symptoms present (eg, joint pain, joint swelling, sicca symptoms, constitutional symptoms) |
Respiratory and rheumatology specialist referral recommended if positive |
|||||||||||||
|
Antibody response to protein and polysaccharide vaccines (tetanus toxoid and pneumococcal) |
To confirm CVID or when specific antibody deficiency suspected (Ig levels normal, recurrent infections) |
Referral to a tertiary bronchiectasis clinic for testing recommended; Ig replacement may be warranted* |
|||||||||||||
|
Cystic fibrosis testing with sweat chloride and/or genetic testing |
If upper lobe predominant bronchiectasis ± consistent phenotype (chronic sinus and gastro-intestinal problems, infertility) |
Referral to a tertiary cystic fibrosis centre recommended |
|||||||||||||
|
PCD screening with nasal nitric oxide, studies of ciliary structure/function |
If consistent clinical phenotype (chronic productive cough since early childhood, recurrent otitis media, infertility) |
Referral to a tertiary PCD centre recommended |
|||||||||||||
|
α-1 antitrypsin levels and phenotype |
If young patient with basal emphysema |
Referral to a tertiary bronchiectasis clinic recommended |
|||||||||||||
|
3 morning sputa or bronchoalveolar lavage for acid-fast bacilli |
If TB or NTM pulmonary disease suspected (fibrocavitary or nodular changes on HRCT chest scan) |
Referral to a tertiary bronchiectasis clinic recommended |
|||||||||||||
|
|
|||||||||||||||
|
CVID = common variable immune deficiency; HRCT = high resolution computed tomography; NTM = non-tuberculous mycobacteria, PCD = primary ciliary dyskinesia; TB = tuberculosis. * See https://www.criteria.blood.gov.au for eligibility criteria for intravenous Ig. |
|||||||||||||||
Box 5 – Approach to the management of stable bronchiectasis in adults
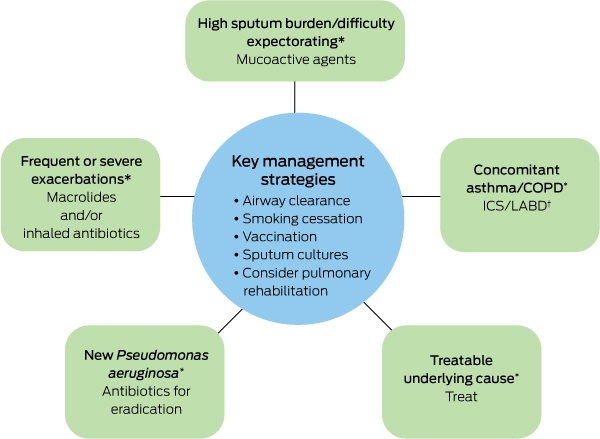
COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroid; LABD = long-acting bronchodilator. * Specialist referral recommended. † ICS/LABD should not be routinely prescribed in patients with bronchiectasis unless they have underlying asthma or COPD.
Box 6 – Indications for specialist review in adult patients with bronchiectasis12
- Patients with Pseudomonas aeruginosa, methicillin-resistant Staphylococcus aureus or mycobacteria on sputum cultures
- Patients with a treatable underlying cause
- Recurrent (≥ 3 per year) or severe exacerbations
- Patients receiving long term antibiotic therapy (oral or nebulised)
- Deteriorating bronchiectasis with declining lung function
- Severe disease
Box 8 – Treatment of severe pulmonary exacerbations of bronchiectasis in adults17
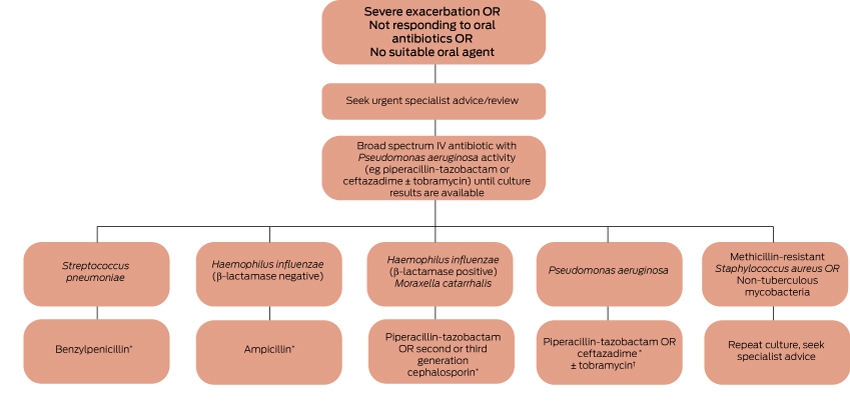
* Guided by antibiotic sensitivities. † There is no evidence at this time that dual therapy for Pseudomonas is superior to monotherapy. Consider dual therapy if the patient has drug-resistant Pseudomonas and no contraindications or interactions.30
Competing interests
Lucy Morgan is Head of the Australian Bronchiectasis Registry Steering Committee.
References
- Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J 2017; 50: 1700629.
- Seitz AE, Olivier KN, Adjemian J, et al. Trends in bronchiectasis among Medicare beneficiaries in the United States, 2000 to 2007. Chest 2012; 142: 432-439.
- Quint JK, Millett ERC, Joshi M, et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. Eur Respir J 2016; 47: 186-193.
- Ringshausen FC, de Roux A, Pletz MW, et al. Bronchiectasis-associated hospitalizations in Germany, 2005-2011: a population-based study of disease burden and trends. PLoS One 2013; 8: e71109.
- Singleton RJ, Valery PC, Morris P, et al. Indigenous children from three countries with non-cystic fibrosis chronic suppurative lung disease/bronchiectasis. Pediatr Pulmonol 2014; 49: 189-200.
- Chang AB, Grimwood K, Mulholland EK, et al. Bronchiectasis in indigenous children in remote Australian communities. Med J Aust 2002; 177: 200-204.
- Bibby S, Milne R, Beasley R. Hospital admissions for non-cystic fibrosis bronchiectasis in New Zealand. N Z Med J 2015; 128: 30-38.
- Australian Consortium for Classification Development. AR-DRG Version 9.0 – final report. 1 Dec 2016. https://www.ihpa.gov.au/sites/g/files/net636/f/publications/ar-drg_v9.0_final_report.pdf (viewed June 2018).
- Serisier DJ, Martin ML, McGuckin MA, et al. Effect of long-term, low-dose erythromycin on pulmonary exacerbations among patients with non–cystic fibrosis bronchiectasis: The BLESS randomized controlled trial. JAMA 2013; 309: 1260-1267.
- Wong C, Jayaram L, Karalus N, Eaton T, Tong C, Hockey H, et al. Azithromycin for prevention of exacerbations in non-cystic fibrosis bronchiectasis (EMBRACE): a randomised, double-blind, placebo-controlled trial. Lancet 2012; 380: 660-667.
- Chang AB, Bell SC, Torzillo PJ, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand. Med J Aust 2015; 202: 21-23.
- Pasteur MC, Bilton D, Hill AT. British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010; 65(Suppl 1): i1-58.
- Tan WC, Hague CJ, Leipsic J, et al. Findings on thoracic computed tomography scans and respiratory outcomes in persons with and without chronic obstructive pulmonary disease: a population-based cohort study. PLoS ONE 2016; 11: e0166745.
- Matsuoka S, Uchiyama K, Shima H, et al. Bronchoarterial ratio and bronchial wall thickness on high-resolution CT in asymptomatic subjects: correlation with age and smoking. Am J Roentgenol 2003; 180: 513-518.
- Gao YH, Guan WJ, Liu SX, et al. Aetiology of bronchiectasis in adults: a systematic literature review. Respirology 2016; 21: 1376-1383.
- Boyton RJ, Altmann DM. Bronchiectasis: current concepts in pathogenesis, immunology, and microbiology. Annu Rev Pathol 2016; 11: 523-554.
- Chang AB, Bell SC, Byrnes CA, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand. Med J Aust 2010; 193: 356-365.
- McDonald CF, Whyte K, Jenkins S, et al. Clinical practice guideline on adult domiciliary oxygen therapy: executive summary from the Thoracic Society of Australia and New Zealand: domiciliary oxygen guideline. Respirology 2016; 21: 76-78.
- Aliberti S, Lonni S, Dore S, et al. Clinical phenotypes in adult patients with bronchiectasis. Eur Respir J 2016; 47: 1113-1122.
- Lee AL, Burge AT, Holland AE. Airway clearance techniques for bronchiectasis. Cochrane Database Syst Rev 2015: CD008351.
- Thoracic Society of Australia and New Zealand. Bronchiectasis toolbox. www.bronchiectasis.com.au (viewed June 2018).
- Lung Foundation Australia. Bronchiectasis. https://lungfoundation.com.au/patient-support/other-lung-conditions/bronchiectasis/ (viewed Mar 2018).
- Haworth CS, Banks J, Capstick T, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017; 72(Suppl 2): ii1-64.
- Spencer S, Felix LM, Milan SJ, et al. Oral versus inhaled antibiotics for non-cystic fibrosis bronchiectasis. Cochrane Database Syst Rev 2017(3): CD012579.
- Kaehne A, Milan SJ, Felix LM, et al. Head-to-head trials of antibiotics for non-cystic fibrosis bronchiectasis. Cochrane Database Syst Rev 2017(3): CD012590.
- Felix LM, Grundy S, Milan SJ, et al. Dual antibiotics for non-cystic fibrosis bronchiectasis. Cochrane Database Syst Rev 2017(1): CD012514.
- Kelly C, Evans DJ, Chalmers JD, et al. Macrolide antibiotics for non-cystic fibrosis bronchiectasis. Cochrane Database Syst Rev 2016(10): CD012406.
- Aksamit TR, O’Donnell AE, Barker A, et al. Adult patients with bronchiectasis: a first look at the US Bronchiectasis Research Registry. Chest 2017; 151: 982-992.
- Hill AT, Haworth CS, Aliberti S, et al. Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research. Eur Respir J 2017; 49: 1700051.
- Abo-Leyah H, Chalmers JD. New therapies for the prevention and treatment of exacerbations of bronchiectasis. Curr Opin Pulm Med 2017; 23: 218-224.
- Wilson R, Aksamit T, Aliberti S, et al. Challenges in managing Pseudomonas aeruginosa in non-cystic fibrosis bronchiectasis. Respir Med 2016; 117: 179-189.
- Brodt AM, Stovold E, Zhang L. Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review. Eur Respir J 2014; 44: 382-393.
- Xu L, Zhang F, Du S, et al. Inhaled antibiotics in non-cystic fibrosis bronchiectasis: a meta-analysis. Pharmazie 2016; 71: 491-498.
- Yang JW, Fan LC, Lu HW, et al. Efficacy and safety of long-term inhaled antibiotic for patients with noncystic fibrosis bronchiectasis: a meta-analysis. Clin Respir J 2016; 10: 731-739.
- Chalmers JD, Smith MP, McHugh BJ, et al. Short- and long-term antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med 2012; 186: 657-665.
- Barker AF, Couch L, Fiel SB, et al. Tobramycin solution for inhalation reduces sputum Pseudomonas aeruginosa density in bronchiectasis. Am J Respir Crit Care Med 2000; 162(2 Pt 1): 481-485.
- Murray MP, Govan JR, Doherty CJ, et al. A randomized controlled trial of nebulized gentamicin in non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med 2011; 183: 491-499.
- Haworth CS, Foweraker JE, Wilkinson P, et al. Inhaled colistin in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection. Am J Respir Crit Care Med 2014; 189: 975-982.
- Barker AF, O’Donnell AE, Flume P, et al. Aztreonam for inhalation solution in patients with non-cystic fibrosis bronchiectasis (AIR-BX1 and AIR-BX2): two randomised double-blind, placebo-controlled phase 3 trials. Lancet Respir Med 2014; 2: 738-749.
- Aksamit T, De Soyza A, Bandel TJ, et al. RESPIRE 2: a phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur Respir J 2018; 51: 1702053.
- De Soyza A, Aksamit T, Bandel T-J, et al. RESPIRE 1: a phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur Respir J 2018; 51: 1702052.
- The European Bronchiectasis Registry. Results from RESPIRE 2 and ORBIT-3 and -4. https://www.bronchiectasis.eu/results-from-respire-2-and-orbit-3-and-4 (viewed June 2018).
- Altenburg J, de Graaff CS, Stienstra Y, et al. Effect of azithromycin maintenance treatment on infectious exacerbations among patients with non–cystic fibrosis bronchiectasis: the BAT randomized controlled trial. JAMA 2013; 309: 1251-1259.
- Zhuo G-Y, He Q, Xiang-Lian L, et al. Prolonged treatment with macrolides in adult patients with non-cystic fibrosis bronchiectasis: meta-analysis of randomized controlled trials. Pulm Pharm Ther 2014; 29: 80-88.
- Wu Q, Shen W, Cheng H, Zhou X. Long-term macrolides for non-cystic fibrosis bronchiectasis: a systematic review and meta-analysis. Respirology 2014; 19: 321-329.
- Yao G-Y, Ma Y-L, Zhang M-Q, Gao Z-C. Macrolide therapy decreases chronic obstructive pulmonary disease exacerbation: a meta-analysis. Respiration 2013; 86: 254-260.
- Haworth CS, Bilton D, Elborn JS. Long-term macrolide maintenance therapy in non-CF bronchiectasis: evidence and questions. Respir Med 2014; 108: 1397-1408.
- Prolonged antibiotic treatment of severe bronchiectasis: a report by a subcommittee of the Antibiotics Clinical Trials (Non-Tuberculous) Committee of The Medical Research Council. Br Med J 1957; 2: 255-259.
- Currie DC, Garbett ND, Chan KL, et al. Double-blind randomized study of prolonged higher-dose oral amoxycillin in purulent bronchiectasis. Q J Med 1990; 76: 799-816.
- Hill SL, Burnett D, Hewetson KA, Stockley RA. The response of patients with purulent bronchiectasis to antibiotics for four months. Q J Med 1988; 66: 163-173.
- Daviskas E, Robinson M, Anderson SD, Bye PTP. Osmotic stimuli increase clearance of mucus in patients with mucociliary dysfunction. J Aerosol Med Pulm Drug Deliv 2002; 15: 331-341.
- Kellett F, Robert NM. Nebulised 7% hypertonic saline improves lung function and quality of life in bronchiectasis. Respir Med 2011; 105: 1831-1835.
- Nicolson CHH, Stirling RG, Borg BM, et al. The long term effect of inhaled hypertonic saline 6% in non-cystic fibrosis bronchiectasis. Respir Med 2012; 106: 661-667.
- Bilton D, Daviskas E, Anderson SD, et al. Phase 3 randomized study of the efficacy and safety of inhaled dry powder mannitol for the symptomatic treatment of non-cystic fibrosis bronchiectasis. Chest 2013; 144: 215-225.
- Bilton D, Tino G, Barker AF, et al. Inhaled mannitol for non-cystic fibrosis bronchiectasis: a randomised, controlled trial. Thorax 2014; 69: 1073-1079.
- O’Donnell AE, Barker AF, Ilowite JS, Fick RB. Treatment of idiopathic bronchiectasis with aerosolized recombinant human DNase I. Chest 1998; 113: 1329-1334.
- Kapur N, Bell S, Kolbe J, Chang AB. Inhaled steroids for bronchiectasis. Cochrane Database Syst Rev 2009(1): CD000996.
- Martínez-García MÁ, Soler-Cataluña JJ, Catalán-Serra P, et al. Clinical efficacy and safety of budesonide-formoterol in non-cystic fibrosis bronchiectasis. Chest 2012; 141: 461-468.
- Wong C, Chang C, Lewis C, et al. Tiotropium treatment for bronchiectasis (ROBUST): a randomized, placebo-controlled, crossover trial. Eur Respir J 2017; 50(Suppl 61).
Linked content
-
MJA Podcast: Dr Simone Visser and Clinical Associate Professor Lucy Morgan
-
MJA InSight: Bronchiectasis: emerging from the shadows
Provenance: Not commissioned; externally peer reviewed.