





Volume 208 - Issue 4
Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders: major depression summary
Authors: Gin S Malhi, Tim Outhred, Amber Hamilton, Philip M Boyce, Richard Bryant, Paul B Fitzgerald, Bill Lyndon, Roger Mulder, Greg Murray, Richard J Porter, Ajeet B Singh and Kristina Fritz
Med J Aust 2018; 208 (4): 175-180. || doi: 10.5694/mja17.00659
Published online: 5 February 2018
Published online: 5 February 2018
New guidelines promote a broader approach to the diagnosis and management of depression
Abstract
Introduction: In December 2015, the Royal Australian and New Zealand College of Psychiatrists published a comprehensive set of mood disorder clinical practice guidelines for psychiatrists, psychologists and mental health professionals. This guideline summary, directed broadly at primary care physicians, is an abridged version that focuses on major depression. It emphasises the importance of shared decision making, tailoring personalised care to the individual, and delivering care in the context of a therapeutic relationship. In practice, the management of depression is determined by a multitude of factors, including illness severity and putative aetiology, with the principal objectives of regaining premorbid functioning and improving resilience against recurrence of future episodes.
Main recommendations: The guidelines emphasise a biopsychosocial lifestyle approach and provide the following specific clinical recommendations:
- Alongside or before prescribing any form of treatment, consideration should be given to the implementation of strategies to manage stress, ensure appropriate sleep hygiene and enable uptake of healthy lifestyle changes.
- For mild to moderate depression, psychological management alone is an appropriate first line treatment, especially early in the course of illness.
- For moderate to severe depression, pharmacological management is usually necessary and is recommended first line, ideally in conjunction with psychosocial interventions.
Changes in management as a result of the guidelines: The management of depression is anchored within a therapeutic relationship that attends to biopsychosocial lifestyle aspects and psychiatric diagnosis. The guidelines promote a broader approach to the formulation and management of depression, with treatments tailored to depressive subtypes and administered with clear steps in mind. Lifestyle and psychological therapies are favoured for less severe presentations, and concurrent antidepressant prescription is reserved for more severe and otherwise treatment-refractory cases.
Globally, depression is now the leading cause of disability. The complexities of the human mind and the lack of a specific treatment target mean that the diagnosis and management of depression are mired in uncertainty. This guideline summary, which has been abstracted from the more comprehensive Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical Practice Guidelines for Mood Disorders,1 accompanies our guideline summary for the treatment of bipolar disorders2 and aims to help clinicians navigate challenging clinical scenarios.
The 2015 mood disorder guidelines1 highlight developments in the management of mood disorders since the previous publication in 2004.3 Key changes include amalgamating evidence-based knowledge with clinical wisdom to generate recommendations applicable to real-world practice, alongside updating treatment options by including new medications and psychological treatments.
This guideline summary tailors care to the individual in the context of a collaborative therapeutic relationship and is directed at doctors with an interest in depression.
Background
With increasing societal and professional awareness, it has become apparent that depression is remarkably common (Box 1, A). It occurs throughout life, with peaks in youth, early adulthood and early old age, and affects both genders.4,5 It is often the backdrop for suicidal thinking and behaviour and occurs alongside many psychiatric and medical illnesses (eg, anxiety, substance abuse, heart disease and thyroid dysfunction) (Box 1, E and F). The emergence of depression is sometimes insidious and the initial symptoms vary markedly. This makes it difficult for patients to recognise they are unwell and consequently many delay seeking treatment — an issue compounded by perceived stigma. Detection and diagnosis are also problematic for health professionals, as patients who eventually present to their family doctor often emphasise their somatic complaints, such as pain and fatigue.
When a diagnosis of depression is suspected, a careful history is necessary to elucidate key symptoms (Box 1, B). Anhedonia and guilt are particularly useful for identifying depression, especially in the context of other illnesses.6 Cognitive symptoms such as problems with memory and concentration, and ruminations involving helplessness and hopelessness are also important. Along with suicidal ideation, these need to be explored carefully.7 The nature and extent of low mood should be documented and ideally assessed using a rating scale (eg, the Hamilton Rating Scale for Depression,8 Kessler Psychological Distress Scale9 or Depression Anxiety Stress Scales10).
Method
The RANZCP appointed a Mood Disorders Committee, independent of any pharmaceutical group, comprising specialists with academic and clinical expertise to develop the clinical practice guidelines for mood disorders.1 The introduction to the full guidelines (the freely accessible version of the full guidelines is available via the RANZCP website at https://www.ranzcp.org/Files/Resources/Publications/CPG/Clinician/Mood-Disorders-CPG.aspx) outlines the scope and methodology of the guideline development process. The Committee synthesised clinical and research evidence from existing depression guidelines using recognised search engines.
The guidelines make two types of recommendations that reflect the reasoning used to formulate advice. First, evidence-based recommendations (EBRs) were formulated using National Health and Medical Research Council (NHMRC) levels of evidence for intervention studies and graded accordingly in the recommendation box (eg, EBR level I, etc).11 Second, consensus-based recommendations (CBRs) were derived through discussion and agreement within the Committee. A CBR was formulated when the existing intervention evidence base was absent, ambiguous or of doubtful clinical impact in the Australian and New Zealand context, and the Committee (based on their clinical and research knowledge and experience) reached consensus on the clinical utility of the recommendation.
Before publication, the draft guidelines developed by the Mood Disorders Committee underwent extensive consultation involving expert and clinical advisers, the public, consumer groups, professional bodies and mood disorders interest groups. Following review, the guidelines were published in the Australian and New Zealand Journal of Psychiatry.1
Recommendations
Clinical recommendations for the management of depression
The guidelines emphasise the importance of recognising the symptoms of depression and making a diagnosis — acknowledging that it is a sophisticated process which involves detailed information gathering, a thorough clinical assessment (including a comprehensive mental state examination) and the careful consideration of corroborative information. This allows the development of a case formulation that fully captures the patients’ problems and frames them within the biopsychosocial and lifestyle model, having identified predisposing, precipitating and perpetuating factors (Box 1, D).1
Depressive disorders usually feature low mood and/or a loss of pleasure (anhedonia), accompanied by somatic and cognitive symptoms (Box 1, B). These symptoms need to be distinguished from normal or appropriate sadness that could arise following adversity. Clinically, the most important signal of depression is functional impairment (depressed individuals are appreciably limited in their ability to perform their normal day-to-day duties).7 There are several subtypes of depression that can be distinguished on the basis of their symptom profiles (frequency/intensity) and duration of episodes.7 This guideline summary focuses on the archetypal diagnosis, major depressive disorder (MDD), because it is the most common community presentation. Other subtypes are important and are discussed in detail in the full guidelines (for the DSM-5 criteria for depressive disorders, see Table 3 in the full guidelines).1 Once detected and properly diagnosed, appropriate management of depression should commence promptly.
The main objective of treatment for MDD is to achieve complete remission of depressive symptoms with full recovery of premorbid functioning. In addition, treatment should reduce associated morbidity and limit disability and risk of self-harm or fatality. This also entails developing resilience to prevent further illness,12-14 and by focusing on the patient’s strengths, engagement with treatment is enhanced. A stepped management summary is shown in Box 1, C.
Step 0: Consider predisposing and lifestyle factors
Once a diagnosis of clinical depression has been formulated, it is important to consider lifestyle factors (poor sleep hygiene, tobacco or illicit drug use) and potential medical causes. A physical screen for medical comorbidities should be conducted (Table 9 in the full guidelines) and, if medically appropriate, medications that can potentially lower mood should be tapered and ceased.
It is also essential to educate the individual about healthy lifestyle habits, such as regular exercise, balanced diet and good sleep hygiene — all of which are protective against the development of depression and are effective treatment strategies.15-19 In addition, any alcohol or drug use should be appropriately managed either before or alongside commencing treatment for depression. This is critical because ongoing significant substance misuse severely limits the benefits of antidepressant and psychological interventions for depression.20-22 Regular review is usually necessary especially at the outset and with follow-up should ideally occur within one week.
Step 1: Consider interventions
Determining the course of treatment
Determining which course of treatment is likely to be most effective depends on a number of factors, including the severity of symptoms and their aetiology. Treatment should be guided by a published manual and tailored to the individual (CBR). In patients with mild to moderate MDD, psychological management should be first line treatment, especially early in the course of illness (EBR level I) (Box 2). Patients who suffer from moderate to severe MDD and illnesses that run a chronic course are likely to require the addition of antidepressant medication, or an alternative combination of psychological and pharmacological treatment (EBR level I). For a full list of recommendations, see Box 3.
Generic psychosocial interventions
At a minimum, it is recommended that psychoeducation be provided and that some form of psychotherapy accompany pharmacotherapy whenever possible. Patients should also be advised to reach out for support beyond their physician, including low intensity interventions (eg, self-help literature, online treatments), social support (eg, consumer support groups, patients’ social networks) and other services as necessary (eg, housing, employment, drugs and alcohol).
Psychological therapy
The various evidence-based psychological treatments are similar in effectiveness, and share a collaborative, skill development focus. Psychological interventions should only be delivered by clinicians trained in the relevant evidence-based approach (CBR). Cognitive behaviour therapy (CBT), the best known and most widely used psychological treatment, aims to modify dysfunctional cognitions and related behaviours presumed to maintain depression.23,24 Interpersonal psychotherapy also has a strong evidence base, and it focuses on interpersonal and role transition issues. Third wave psychotherapies such as mindfulness-based CBT and acceptance and commitment therapy that focus on present moment experience as the locus of change have also been found to be useful25 (Table 12 in the full guidelines). Ideally, physicians should refer patients for specific therapies based on symptoms and patient preference, but in practice, access to suitably trained psychological therapists is often the primary determinant.
Pharmacotherapy
The decision to treat an individual patient with an antidepressant remains very much a matter of clinical judgement. This is because there are no reliable predictors of treatment response. When commencing antidepressant therapy, clinical response and side effects should be closely monitored from the outset (CBR). In general, newer (second and third generation) antidepressants are safer first line options.26 Selective serotonin reuptake inhibitors (SSRIs) are often used first because they are safe, moderately well tolerated and reasonably efficacious. Serotonin–norepinephrine reuptake inhibitors and noradrenergic and specific serotonergic antidepressants are just as effective but often have more side effects. Noradrenaline reuptake inhibitors and noradrenaline–dopamine reuptake inhibitors have been shown to be less effective than other antidepressants and should only be considered when tolerability is a key concern. Traditional (first generation) antidepressants (tricyclic antidepressants) and monoamine oxidase inhibitors appear to have greater efficacy, but tolerability and safety concerns, especially in overdose, usually relegate them to second or third line treatment26 (Table 13 in the full guidelines).
An adequate trial of an antidepressant should be a minimum of 3 weeks at the recommended therapeutic dose (EBR level III). In most instances, a clinical response emerges within the first 2 weeks of treatment; early and regular follow-up is therefore important. Regular review is also critical because of the potential for antidepressants, particularly SSRIs, to trigger suicidal thoughts and behaviour — especially in adolescents and young adults.27 Clinicians should therefore advise young patients and their families of the small chance of suicidal thoughts emerging during the early phase of treatment with SSRIs and monitor all patients for their emergence or worsening during the first 2–4 weeks of treatment. Co-prescribing a low dose of a benzodiazepine for the first 1–2 weeks of treatment may reduce the activation that can occur upon initiation of an SSRI (CBR).
Step 2: Consider treatment strategies
Combination of psychological therapy and pharmacotherapy
If no improvement is apparent within the first 3 weeks of adequate treatment, a combined treatment approach is advocated. This applies particularly to moderate to severe MDD (EBR level I) and chronic depression (EBR level I).28-34 It is also important to review the diagnosis and confirm treatment adherence, especially if the patient has not fully responded.
Dose increase
After ensuring the patient has been taking medication as prescribed, a dose increase is the most expedient strategy to trial (CBR). However, increasing the antidepressant dose beyond the recommended maximum is only useful for some, not all, antidepressants and should only be considered if the patient has clearly demonstrated a partial response (CBR).35
Switching and substitution
In primary care, most patients are prescribed an SSRI antidepressant as first line therapy. Patients who do not tolerate the initial SSRI often tolerate and benefit from a second SSRI.36 It is recommended that initially patients use a lower dose of the second SSRI, and in some instances it may be necessary to taper the first SSRI for a longer period (CBR) (eg, switching from citalopram to escitalopram can be immediate, but switching from fluoxetine to another antidepressant usually requires a wash-out period of at least a week before commencing the second agent at a lower dose to avoid the risk of serotonergic syndrome). However, if the patient is not responsive to the initial SSRI, switching out of class to a serotonin–norepinephrine reuptake inhibitor (eg, venlafaxine or duloxetine), noradrenaline–dopamine reuptake inhibitor or tricyclic antidepressant is recommended (CBR).37,38 Switching is an important strategy but should only be considered once an adequate trial at an adequate dose has been achieved.39,40 The full guidelines provide a comprehensive overview of switching strategies.
Augmentation
If the patient does not respond to the initial antidepressant or to an increase in dosage, another strategy to consider is to augment with either lithium or a second generation antipsychotic medication (EBR level I). Predictors of likely response to lithium augmentation include recurrent major depression with more than three recurrences and a family history of bipolar or unipolar depression in a first degree relative.41 In the case of lithium augmentation, if there is no response within 7–10 days (and a therapeutic serum level has been achieved), alternative strategies should be considered.42 However, caution should be exercised when discontinuing the use of lithium, because abrupt withdrawal can increase the likelihood of relapse.43 See the full guidelines for more information about augmentation strategies.
Specialist involvement
Once an effective dose has been achieved, remission usually requires 6 weeks of continuous treatment. However, there are many patients who do not respond to multiple trials of treatment; such patients should be promptly referred to a psychiatrist — ideally, a mood disorder specialist.
For the management of treatment-resistant depression, some specialist centres may be able to offer repetitive transcranial magnetic stimulation, which may be trialled but costs considerably more than medication strategies and is no more effective.44
Step 3: Consider electroconvulsive therapy
Physical treatment
Electroconvulsive therapy is a safe and effective treatment for the more severe forms of depression (EBR level I).45 In practice, electroconvulsive therapy is usually reserved for patients who have not responded to several trials of medication; however, it is recommended first line treatment for extremely severe or psychotic depression, particularly when the patient has exceptionally high levels of distress, refuses to eat or drink and/or poses a considerable suicide risk (EBR level I) (Box 3).
Other considerations
Outpatient v inpatient
In most cases, depression can be managed on an outpatient basis, but patients with severe symptoms may require inpatient treatment under the care of a psychiatrist. Hospitalisation of a depressed patient is a matter of clinical judgement (Table 10 in the full guidelines), and is most often considered when patients have suicidal intent (CBR). Physical risk from malnourishment, dehydration and medical and psychiatric comorbidities (Box 1, E and F), such as severe medical ill health or substance misuse, may warrant inpatient treatment.
General practitioner v psychiatrist
Many patients first present to the GP with somatic symptoms or possibly low mood. A key role of the GP is to determine the severity and complexity of emotional symptoms, make an accurate diagnosis, and decide if referral to a psychiatrist or psychologist is needed. For mild depressive symptoms and in the absence of suicidality or diagnostic uncertainty, management by the GP is usually sufficient with or without added psychiatric input (CBR). However, where there is diagnostic complexity, a high risk of self-harm, non-response or severe debility, prompt referral for psychiatric assessment is advised (CBR).
Special considerations
The guidelines acknowledge that the clinical picture of mood disorders is highly variable, but that certain groups of features form characteristic syndromes or subtypes for which they provide guidance for diagnosis and management.46,47 Depression may also present with psychiatric or medical comorbidities such as anxiety,48,49 substance misuse,21,50 and personality disorders.51,52
Conclusion
The clinical practice guidelines for mood disorders provide updated and relevant information for physicians (including GPs) regarding the management of depression. They highlight the importance of tailoring care to the individual and creating a collaborative therapeutic relationship, while outlining key considerations for long term treatment strategies. The advice provided in the guidelines should enable clinicians to successfully navigate the complexities of managing depression.
Box 1 – An overview of depression and its treatment*
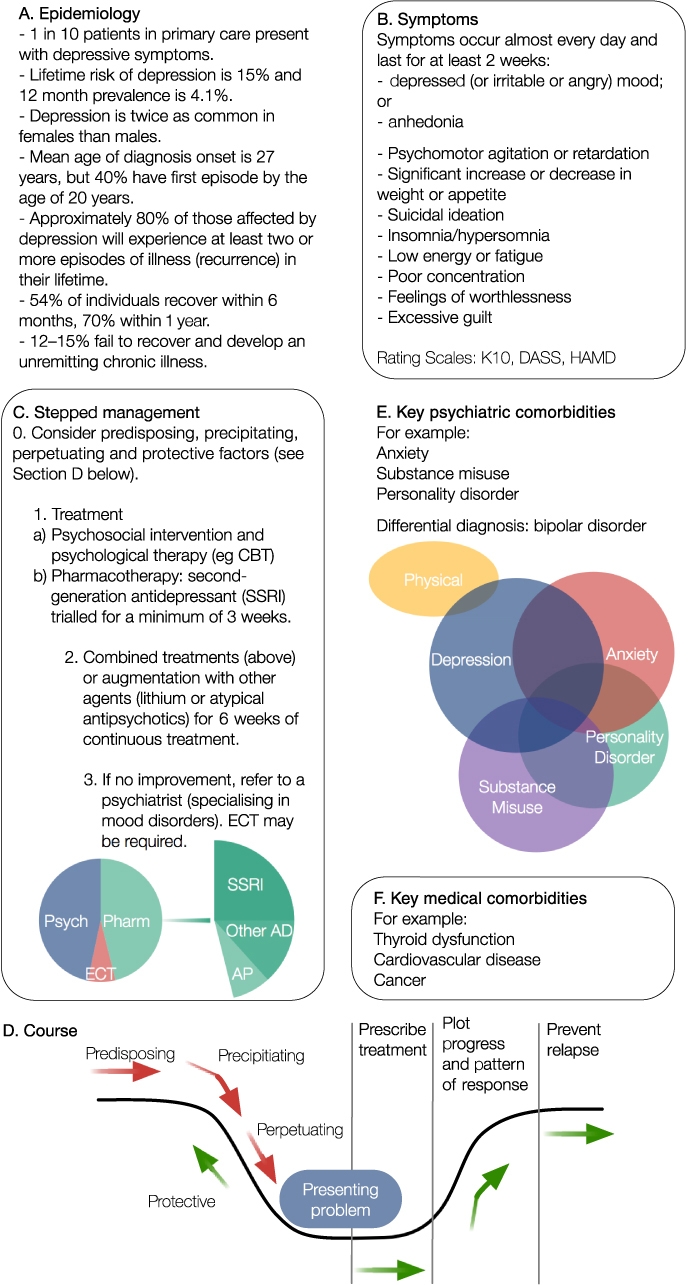
A: Epidemiology: depression is common in the community and the majority of patients present to GPs with depressive symptoms. B: Symptoms: symptoms of depression can be captured using rating scales (Kessler Psychological Distress Scale [K10], Depression Anxiety Stress Scales [DASS] and Hamilton Rating Scale for Depression [HAMD]). C: Stepped management: major depressive disorder is an episodic recurrent illness and the goal of management is to treat the episodes and prevent future recurrence. Major depressive disorder is primarily managed with psychological therapies (Psych) and medications (Pharm). Severe or unremitting episodes may require electroconvulsive therapy (ECT). First line treatments may include cognitive behaviour therapy (CBT) and a selective serotonin reuptake inhibitor (SSRI). In some patients, alternative antidepressants (Other AD) and antipsychotics (AP) may need to be employed. D: Course: the steps involved in formulation include examining the presenting problem and identifying any predisposing, precipitating and perpetuating factors. Once treatment has been prescribed, the progress and pattern of response should be plotted to map improvement and ensure future relapse is prevented. The protective factors that can help to prevent episodes and limit illness progression should also be identified. E: Key psychiatric comorbidities: patients with major depressive disorder often have comorbid anxiety. In these instances CBT and SSRIs are effective. Comorbidities such as substance misuse and personality disorder usually require specialist interventions. F: Key medical comorbidities: patients with major depressive disorder commonly present with physical comorbidities. Thyroid dysfunction is often a cause of mood disturbance, and cardiovascular disease (CVD) or cancer can sometimes precipitate the development of major depressive disorder. * Adapted with permission from Malhi et al.1
Box 2 – Management of major depressive disorders*
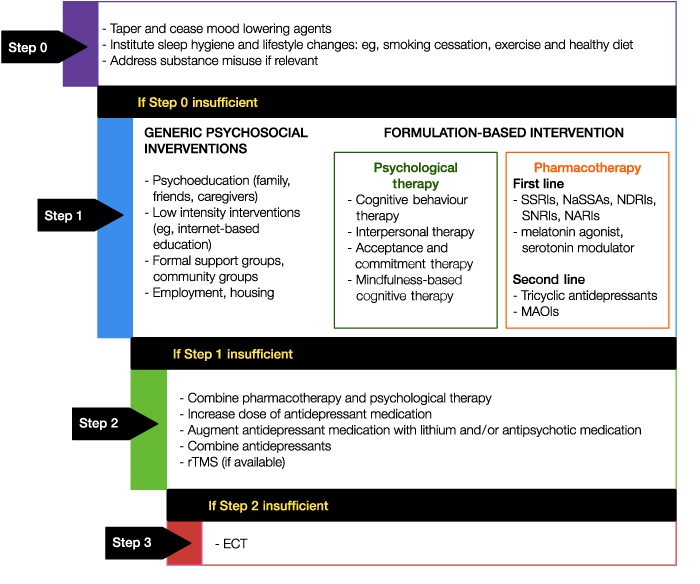
ECT = electroconvulsive therapy; MAOI = monoamine oxidase inhibitor; NARI = noradrenaline reuptake inhibitor; NaSSA = noradrenergic and specific serotonergic antidepressant; NDRI = noradrenaline–dopamine reuptake inhibitor; rTMS = repetitive transcranial magnetic stimulation; SNRI = serotonin–norepinephrine reuptake inhibitors; SSRI = selective serotonin reuptake inhibitor. Schematic illustration of stepwise management of major depressive disorder. In Step 1 a whole host of interventions and therapies need to be considered, and choice of treatment should be based on individual formulation. Note the various steps are not necessarily sequential and in some instances treatment may commence with options selected from Step 2 or Step 3. * Reproduced with permission from Malhi et al.1
Box 3 – Treatment recommendations for depressive disorders*
|
Treatment recommendation |
Grade |
||||||||||||||
|
|
|||||||||||||||
|
Only clinicians trained in a relevant evidence-based approach should deliver psychological interventions |
CBR |
||||||||||||||
|
Patients with mild to moderate depression should be offered one of the evidence-based psychotherapies as first line treatment |
EBR level I |
||||||||||||||
|
Patients with moderate to severe depression should be offered combined pharmacotherapy and psychotherapy as first line treatment |
EBR level I |
||||||||||||||
|
Patients with chronic depressive disorders should be offered combined psychotherapy and pharmacotherapy as first line treatment |
EBR level I |
||||||||||||||
|
An adequate trial of antidepressant therapy for major depressive disorders should be a minimum of 3 weeks at the recommended therapeutic dose using a suitable medication |
EBR level III |
||||||||||||||
|
Electroconvulsive therapy is a safe and effective treatment for more severe presentations of depression and should be considered first line for psychotic depression, or when an immediate response is necessary |
EBR level I |
||||||||||||||
|
|
|||||||||||||||
|
CBR = consensus-based recommendation; EBR = evidence-based recommendation (based on National Health and Medical Research Council levels of evidence10).* Adapted with permission from Malhi et al.1 |
|||||||||||||||
Competing interests
Gin Malhi has received grant or research support from Australian Rotary Health, the NHMRC, the American Foundation for Suicide Prevention, NSW Health, Ramsay Health, the University of Sydney, AstraZeneca, Eli Lilly, Organon, Pfizer, Servier and Wyeth; has been a speaker for AstraZeneca, Eli Lilly, Janssen-Cilag, Lundbeck, Pfizer, Ranbaxy, Servier and Wyeth; and has been a consultant for AstraZeneca, Eli Lilly, Janssen-Cilag, Lundbeck and Servier. Phillip Boyce has received consultation fees, sponsorship and speaker fees from Servier; is a member of the advisory board for Lundbeck, Eli Lilly, AstraZeneca and Janssen; has received speaker fees from Lundbeck, AstraZeneca and Janssen; and has received funding for a clinical trial from Brain Resource Company. Richard Bryant has received an NHMRC Program Grant and Project Grant. Paul Fitzgerald is supported by an NHMRC Practitioner Fellowship Grant; and has received equipment for research from MagVenture A/S, Medtronic Ltd, Neuronetics and Brainsway Ltd, and funding for research from Neuronetics. He is on scientific advisory boards for Bionomics Ltd and LivaNova and is a founder of TMS Clinics Australia. Bill Lyndon has received personal fees from Lundbeck Australia, AstraZeneca and Eli Lilly Australia. Greg Murray has received an NHMRC Project Grant and personal fees from Servier and CSL Biotherapies. Ajeet Singh has received personal fees from Servier Australia and Lundbeck Australia; has received a grant from Pfizer Australia; has equity in ; is the founder and owner of website; and has a patent on the Antidepressant Pharmacogenetics Report.
Acknowledgements
The development of the clinical practice guidelines for mood disorders was supported and funded by the RANZCP.
References
- Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry 2015; 49: 1087-1206.
- Malhi GS, Outhred T, Morris G, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders: bipolar disorder summary. Med J Aust 2018; https://doi.org/10.5694/mja17.00658 [Epub ahead of print].
- Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Depression. Australian and New Zealand clinical practice guidelines for the treatment of depression. Aust N Z J Psychiatry 2004; 38: 389-407.
- Alonso J, Angermeyer MC, Bernert S, et al. Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl 2004; 109(420): 21-27.
- Backenstrass M, Frank A, Joest K, et al. A comparative study of nonspecific depressive symptoms and minor depression regarding functional impairment and associated characteristics in primary care. Compr Psychiatry 2006; 47: 35-41.
- Nicholas MK, Coulston CM, Asghari A, Malhi GS. Depressive symptoms in patients with chronic pain. Med J Aust 2009; 190: 66.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: APA, 2013.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23: 56.
- Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med 2002; 32: 959-976.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther 1995; 33: 335-343.
- National Health and Medical Research Council. Additional levels of evidence and grades for recommendations for developers of guidelines. 2009. https://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/developers/nhmrc_levels_grades_evidence_120423.pdf (viewed Dec 2017).
- Malhi G, Hitching R, Coulston C, et al. Individualized management of unipolar depression. Acta Psychiatr Scand Suppl 2013; 127(443): 1-5.
- Friedman AK, Walsh JJ, Juarez B, et al. Enhancing depression mechanisms in midbrain dopamine neurons achieves homeostatic resilience. Science 2014; 344: 313-319.
- Oldehinkel AJ, Ormel J, Verhulst FC, Nederhof E. Childhood adversities and adolescent depression: a matter of both risk and resilience. Dev Psychopathol 2014; 26(4 Pt 1): 1067-1075.
- Asarnow LD, Soehner AM, Harvey AG. Basic sleep and circadian science as building blocks for behavioral interventions: a translational approach for mood disorders. Behav Neurosci 2014; 128: 360.
- Harvey AG. Sleep and circadian functioning: critical mechanisms in the mood disorders? Annu Rev Clin Psychol 2011; 7: 297-319.
- Malhi G, Kuiper S. Chronobiology of mood disorders. Acta Psychiatr Scand Suppl 2013; 128(444): 2-15.
- Bridle C, Spanjers K, Patel S, et al. Effect of exercise on depression severity in older people: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry 2012; 201: 180-185.
- Hare BD, Beierle JA, Toufexis DJ, et al. Exercise-associated changes in the corticosterone response to acute restraint stress: evidence for increased adrenal sensitivity and reduced corticosterone response duration. Neuropsychopharmacology 2014; 39: 1262-1269.
- Worthington J, Fava M, Agustin C, et al. Consumption of alcohol, nicotine, and caffeine among depressed outpatients: relationship with response to treatment. Psychosomatics 1996; 37: 518-522.
- Torrens M, Fonseca F, Mateu G, Farré M. Efficacy of antidepressants in substance use disorders with and without comorbid depression: a systematic review and meta-analysis. Drug Alcohol Depend 2005; 78: 1-22.
- Roy K, Parker G, Mitchell P, Wilhelm K. Depression and smoking: examining correlates in a subset of depressed patients. Aust N Z J Psychiatry 2001; 35: 329-335.
- National Institute for Health and Care Excellence. Depression in adults: recognition and management. Clinical guideline CG90. London: NICE, 2009. https://www.nice.org.uk/guidance/cg90/resources/depression-in-adults-recognition-and-management-pdf-975742636741 (viewed Dec 2017).
- Parikh SV, Segal ZV, Grigoriadis S, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. II. Psychotherapy alone or in combination with antidepressant medication. J Affect Disord 2009; 117: S15-S25.
- Hunot V, Moore T, Caldwell D, et al. Mindfulness-based ‘third wave’ cognitive and behavioural therapies versus other psychological therapies for depression. Cochrane Database Syst Rev 2010; (9) CD008704.
- Peretti S, Judge R, Hindmarch I. Safety and tolerability considerations: tricyclic antidepressants vs. selective serotonin reuptake inhibitors. Acta Psychiatr Scand Suppl 2000; 101(403): 17-25.
- Möller H-J, Baldwin DS, Goodwin G, et al. Do SSRIs or antidepressants in general increase suicidality? Eur Arch Psychiatry Clin Neurosci 2008; 258: 3-23.
- Cuijpers P, Dekker J, Hollon SD, Andersson G. Adding psychotherapy to pharmacotherapy in the treatment of depressive disorders in adults: a meta-analysis. Nord J Psychiatry 2009; 70: 1219-1229.
- De Maat SM, Dekker J, Schoevers RA, De Jonghe F. Relative efficacy of psychotherapy and pharmacotherapy in the treatment of depression: a meta-analysis. Psychother Res 2006; 16: 566-578.
- Manber R, Kraemer HC, Arnow BA, et al. Faster remission of chronic depression with combined psychotherapy and medication than with each therapy alone. J Consult Clin Psychol 2008; 76: 459-467.
- Pampallona S, Bollini P, Tibaldi G, et al. Combined pharmacotherapy and psychological treatment for depression: a systematic review. Arch Gen Psychiatry 2004; 61: 714-719.
- Schramm E, Schneider D, Zobel I, et al. Efficacy of interpersonal psychotherapy plus pharmacotherapy in chronically depressed patients. J Affect Disord 2008; 109: 65-73.
- Schramm E, van Calker D, Dykierek P, et al. An intensive treatment program of interpersonal psychotherapy plus pharmacotherapy for depressed inpatients: acute and long-term results. Am J Psychiatry 2007; 164: 768-777.
- Simon J, Pilling S, Burbeck R, Goldberg D. Treatment options in moderate and severe depression: decision analysis supporting a clinical guideline. Br J Psychiatry 2006; 189: 494-501.
- Malhi G, Adams D, Porter R, et al. Clinical practice recommendations for depression. Acta Psychiatr Scand Suppl 2009; 119(439): 8-26.
- Mars B, Heron J, Gunnell D, et al. Prevalence and patterns of antidepressant switching among primary care patients in the UK. J Psychopharmacol 2017; 31: 553-560.
- Ruhe HG, Huyser J, Swinkels JA, Schene AH. Switching antidepressants after a first selective serotonin reuptake inhibitor in major depressive disorder: a systematic review. J Clin Psychiatry 2006; 67: 1836-1855.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354: 1231-1242.
- Malhi GS, Hamilton A, Morris G, et al. Optimisation of adherence and discontinuation practices for maintenance antidepressant therapy. Aust N Z J Psychiatry 2017; 51: 403-405.
- Bschor T, Baethge C. No evidence for switching the antidepressant: systematic review and meta-analysis of RCTs of a common therapeutic strategy. Acta Psychiatr Scand 2010; 121: 174-179.
- Sugawara H, Sakamoto K, Harada T, Ishigooka J. Predictors of efficacy in lithium augmentation for treatment-resistant depression. J Affect Disord 2010; 125: 165-168.
- Malhi GS, Gessler D, Fritz K, et al. Recommendations in international clinical practice guidelines for lithium therapy of bipolar disorder. In: Mahli GS, Masson M, Bellivier F, editors. The science and practice of lithium therapy. Cham: Springer, 2017; pp 189-209.
- Bauer M, Bschor T, Kunz D, et al. Double-blind, placebo-controlled trial of the use of lithium to augment antidepressant medication in continuation treatment of unipolar major depression. Am J Psychiatry 2000; 157: 1429-1435.
- Gaynes BN, Lloyd SW, Lux L, et al. Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis. J Clin Psychiatry 2014; 75: 477-489.
- Carney S, Cowen P, Dearness K, et al. Efficacy and safety of electroconvulsive therapy in depressive disorders: A systematic review and meta-analysis. Lancet 2003; 361: 799.
- Lyndon B, Parker G, Morris G, et al. Is atypical depression simply a typical depression with unusual symptoms. Aust N Z J Psychiatry 2017; 51: 868-871.
- Parker G, Bassett D, Outhred T, et al. Defining melancholia: a core mood disorder. Bipolar Disord 2017; 19: 235-237.
- Cape J, Whittington C, Buszewicz M, et al. Brief psychological therapies for anxiety and depression in primary care: meta-analysis and meta-regression. BMC Med 2010; 8: 38.
- Stein DJ, Picarel-Blanchot F, Kennedy SH. Efficacy of the novel antidepressant agomelatine for anxiety symptoms in major depression. Hum Psychopharmacol 2013; 28: 151-159.
- Silins E, Copeland J, Dillon P. Qualitative review of serotonin syndrome, ecstasy (MDMA) and the use of other serotonergic substances: hierarchy of risk. Aust N Z J Psychiatry 2007; 41: 649-655.
- Mulder RT, Joyce PR, Luty SE. The relationship of personality disorders to treatment outcome in depressed outpatients. J Clin Psychiatry 2003; 64: 259-264.
- Newton-Howes G, Tyrer P, Johnson T, et al. Influence of personality on the outcome of treatment in depression: systematic review and meta-analysis. J Pers Disord 2014; 28: 577-593.
Linked content
-
Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders: bipolar disorder summary
-
MJA InSight: New guidelines for mood disorders in primary care
-
MJA Podcast: Distinguished Professor Gin Malhi
Provenance: Not commissioned; not externally peer reviewed.
Reorienting Allied Health Into Community-Based Care for People Experiencing Trauma and Social Disadvantage
Simon Rosenbaum, Grace McKeon, Gulsah Kurt, Oscar Lederman, Kemi Wright, Sabuj Kanti Mistry, Jackie E. Curtis, Philip B. Ward, Zachary Steel, Hamish Fibbins, Rachel Morell, Melissa C. Eaton, Andrew Watkins, Ben Harris-Roxas, Brendan Goodger, Eleanor Beck, Megan Teychenne, Joseph Firth, Davy Vancampfort, David Burns, Russell Roberts, Tristan Favaloro, Danielle Weber, Rosanna Barbero, Vasili Maroulis, Melissa Holmes, Stefan Mackenzie, Chiara Mastrogiovanni, Afsana Anwar, Uzma Choudhry, Catherine Sherrington, Jane Currie, Thomas Gadsden, Scott Teasdale
Stigmatising Attitudes Towards People With Depression, Bipolar Disorder, Borderline Personality, ADHD and Early and Long-Term/Untreated Schizophrenia: Representative Survey of Australian Adults
Amy J. Morgan, Anna M. Ross, Gayle McNaught, Rachel Green, Nicola J. Reavley
Psychosocial Hazards for Healthcare Workers: Supporting the Second Victim Also Helps the Primary Victims
Sarah Michael
Supporting Population Mental Health in the Wake of Mass Tragedies
Susan J. Rees, Derrick M. Silove
In the Wake of the National Suicide Prevention Strategy 2025–2035: Suicide Prevention in Type 1 Diabetes
Rigel Paciente, Keely Bebbington, Alix Woolard, Helen Milroy
The risk of death after hospitalisation following intentional self‐poisoning: a retrospective observational study (PAVLOVA‐2)
Firouzeh Noghrehchi, Nicholas A Buckley, Rose Cairns