





Volume 206 - Issue 2
Influence of birth month on the probability of Western Australian children being treated for ADHD
Authors: Martin Whitely, Leanne Lester, John Phillimore and Suzanne Robinson
Med J Aust 2017; 206 (2): 85. || doi: 10.5694/mja16.00398
Published online: 6 February 2017
Published online: 6 February 2017
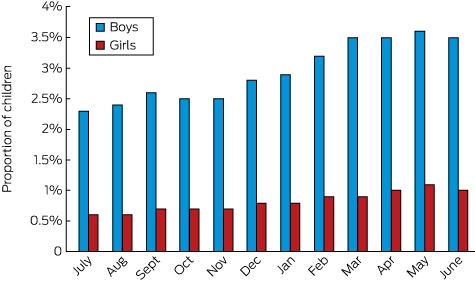
Younger children in school classes are more likely to receive a stimulant medication
Four international studies have found that the youngest children in a school class are more likely than their classmates to receive pharmacological treatment for attention deficit/hyperactivity disorder (ADHD).1-4 We investigated whether this late birth date effect applies to children in Western Australia. We compared the proportions of WA children born in the early and late months of a recommended school-year intake who received at least one Pharmaceutical Benefits Scheme prescription for an ADHD medication in 2013 (Box).
An estimated population of 311 384 children was included in our study, analysed by year and month of birth, sex, and in two 5-year bands: children aged 6–10 years (born July 2003 – June 2008) and children aged 11–15 years (born July 1998 – June 2003). A total of 5937 children (1.9%) received medication for ADHD; the proportion of boys receiving medication (2.9%) was higher than that of girls (0.8%).
Among children aged 6–10 years, those born in June (the last month of the recommended school-year intake) were about twice as likely to have received ADHD medication than those born in the first intake month (the previous July); the relative risks (RRs) were 1.93 for boys (95% confidence interval [CI], 1.53–2.38) and 2.11 for girls (95% CI, 1.57–2.53). For children aged 11–15 years, the effect was less marked, but still significant (RR: boys, 1.26; 95% CI, 1.03–1.52; girls, 1.43; 95% CI, 1.15–1.76). The RRs for the combined group (aged 6–15 years) were 1.52 (95% CI, 1.30–1.73) for boys and 1.73 (95% CI, 1.42–1.94) for girls. Similar differences were found when comparing children born in the first 3 (or 6) months and the last 3 (or 6) months of the school-year intake. These results are consistent with those of previous international studies.
As the data were de-identified, it was impossible to identify which students had commenced school outside their recommended starting year. However, in contrast to other mainland Australian states, fewer than 2% of children in WA start school outside the recommended school-year intake. Delayed entry is most common for children born in June; our study is therefore likely to underestimate the effect of birth date. Further research in states with greater flexibility for parents in deciding their child’s school starting age would help determine whether a broader age spread in school classes is associated with a reduction or increase in any late birthday effect on ADHD medication status.
Frances, who led the DSM-IV development taskforce of the American Psychiatric Association, argued that similar findings in North America indicated that developmental immaturity is mislabelled as a mental disorder and unnecessarily treated with stimulant medication. While he considers ADHD a legitimate diagnosis, he asserted that it is overdiagnosed and overmedicated, estimating that a “diagnostic rate of around 2% … would best balance harms and benefits”.5
The prescribing rate for children in our study was 1.9%, comparable with that reported by a Taiwanese study (1.6%).4 The late birth date effects identified in WA and Taiwan were of similar strength to those in the three North American studies, where the reported ADHD medication prescribing rates for the periods analysed were at least twice as high (4.5%,1 5.8%,2 3.6%3). This indicates that even at relatively low rates of prescribing there are significant concerns about the validity of ADHD as a diagnosis.
Competing interests
No relevant disclosures.
References
- Elder TE. The importance of relative standards in ADHD diagnoses: evidence based on exact birth dates. J Health Econ 2010; 29: 641-656.
- Evans WN, Morrill MS, Parente ST. Measuring inappropriate medical diagnosis and treatment in survey data: the case of ADHD among school-age children. J Health Econ 2010; 29: 657-673.
- Morrow RL, Garland J, Wright JM, et al. Influence of relative age on diagnosis and treatment of attention-deficit/hyperactivity disorder in children. CMAJ 2012; 184: 755-762.
- Chen MH, Lan WH, Bai YM, et al. Influence of relative age on diagnosis and treatment of attention-deficit/hyperactivity disorder in Taiwanese children. J Pediatr 2016; 172: 162-167.e1.
- Frances A. Don’t throw out the baby out with the bathwater. Aust N Z J Psychiatry 2015; 49: 577.
Linked content
-
MJA InSight: Immature kids being misdiagnosed with ADHD
-
The diagnostic validity of mental health diagnoses in children
Hospital-Admitted Injection-Related Infections Among Incarcerated People Who Inject Drugs in Australia: A Retrospective Cohort Study
Andrew Palmer, Matthew Carter, Jeremy Yeo, Cecilia Shim, Jason Connor, Jeremy Hayllar, Gerald Holtmann, Naomi Moy, Elliott G. Playford, Naomi Runnegar, Paul J. Clark
The Management of Withdrawal From Alcohol and Other Drugs in Australian Custodial Settings: A Consensus Statement
Grace FitzGerald, Jocelyn Chan, Jon Cook, Mark Stoove, Michael Curtis, Suzanne Nielsen, Rebecca J. Winter, Thileepan Naren
Impact of Prescription Drug Monitoring Program Implementation on Rates and Characteristics of People Seeing Multiple Prescribers in Primary Care: A Controlled Interrupted Time-Series Analysis
Louisa Picco, Monica Jung, Grant Russell, Samanta Lalic, Mahbod A. Fini, Dan I. Lubman, Rachelle Buchbinder, Ting Xia, Suzanne Nielsen
Early Cessation of Acetylcysteine Treatment After Paracetamol Overdose (NACSTOP 2): A Non-Inferiority Randomised Controlled Trial
Anselm Wong, Richard McNulty, Sarah E. Hodgson, Naren Gunja, Andis Graudins
The risk of death after hospitalisation following intentional self‐poisoning: a retrospective observational study (PAVLOVA‐2)
Firouzeh Noghrehchi, Nicholas A Buckley, Rose Cairns
Opioids and the challenges of managing chronic non‐cancer pain in rural Australia: a qualitative study
Jessica A Thomas, Jill Benson, Philip Davidson, Paul R Ward