




There is a growing focus on the central role of primary care in providing high-quality, accessible, and cost-effective care for international communities. However, maximising the reach and uptake of evidence into primary care policy and practice continues to be a major challenge and a major focus in health reform.1-4 Research translation must ideally be directed in a bottom-up fashion from the community, through effective and consultative partnerships at every stage.5 This demands a “refocus” on the way we conduct health services research,6,7 requiring that strategic partnerships with influential end users are formed early in the research process and nurtured throughout the entire development and implementation journey.
In an effort to maximise investment in research, funding bodies and governments are increasingly working with the academic sector to strengthen partnerships with industry, society and end users of the research to improve the productivity of the sector.8-11 In response, researchers have increasingly adopted approaches such as translational research,12 implementation research,13 and community-based participatory methods14 to facilitate uptake of research findings into health policy and practice.15,16 Although these terms emphasise the use of research in “real-world” settings, they ultimately remain researcher-driven approaches. Thus they may fail to engage the end users of the research (patients, clinicians, and other key stakeholders within health care systems) adequately, may not recognise stakeholder and end user values, and so, may limit effective translation into policy and practice.12 In many cases, the researcher may lack insight into the end users’ specific needs and values in the all-important development phase, making the research outcomes difficult to implement and often unsustainable in the real-world setting.16
Over the past decade, the business sector has witnessed the transformation of multi-million dollar enterprises through the adoption of the “value co-creation paradigm”.17 This paradigm includes important concepts, innovative approaches and key principles, within an overarching framework. Value co-creation is focused on creating value with, and for, multiple stakeholding individuals through regular interactions and value-creating processes.17 These, in turn, create opportunities for increasing innovation, productivity and co-created outcomes of value for the end users, the community at large and the economy.17 This approach is now gaining momentum outside the business world, where it has been used to increase innovation within the public sector to create new joint value.18 There is also a growing literature on health value co-creation and the benefits of consumer value co-creation in the health sector.19-22
In 2011, our Centre of Research Excellence (CRE) in Building Primary Care Quality, Performance and Sustainability was established through a partnership between the University of Queensland and some of Australia’s most influential primary care organisations.23 We used the value co-creation approach to encourage innovation, unify partner capability and maximise the impact of our complex program of research.17,24 In this article, we describe the underpinning principles of value co-creation, the benefits of using this approach, lessons learned and strategies to achieve value co-creation in primary care services research.
A new vision for value co-creation
Value co-creation introduces a new vision of value creation through a shift in thinking about potential co-creators of value, the value networks, and the entire value of ecosystems.25 Value co-creation also requires a redefining of the way an organisation or group engages individuals internally (employees, teams, departments) and externally (suppliers, partners, and other stakeholders) through a process of value creation and engagement in enriched experiences to design new products and services, transform management systems, increase innovation, productivity and returns on investment.24 Strategy is the art of creating value26-28 and, in a co-creative research enterprise, the central focus of the strategy becomes making choices about where and how to co-create value with stakeholders and end users of the research (Box 1).
Co-creation expands the creation of value in three ways: (i) value as enacted through co-creative interactions; (ii) value as exemplified experiences; and, (iii) value as emerging from strategic stakeholder engagement through diverse collaborations across multiple sectors and evolvable ecosystems of capabilities (Box 2).17 Key steps and principles that capture the essence of implementing value co-creation are described below. In Box 3, we provide a case study that illustrates the application of the six key steps to the development of a quality improvement tool for primary care, one of the centrepieces of our CRE program.
Value co-creation steps
1. Strategically engaging stakeholders in creating value together
The first step in any co-creative initiative is to identify key stakeholders and end users who can take part in the co-creation efforts. Value co-creation demands that organisations and individuals reach out to different groups, enterprises or sectors so they can co-create new knowledge together, thus generating more value.17,24 A deeper collaboration with multiple influential stakeholders increases the pool of resources, competencies and capabilities, which accelerates value creation opportunities for all.17,29 With this in mind, the research team must identify and invite research stakeholders, including influential clinical organisations, policy makers, funders and other end users to take part in the co-creation journey from inception.
2. Identifying and supporting champions
Over time, influential co-creation champions need to be identified and supported within all involved enterprises, ecosystems and stakeholder organisations to increase the chance of success of the co-creative initiative.17,29 Change is challenging, and using new approaches to innovation can be confronting to those accustomed to following traditional processes. As the aim of value co-creation is to embed collaborative, ongoing, successful relationships between stakeholders, so champions of the new approach are essential to lever and maintain cultural change in both research, funding, policy and end user groups.
3. Purposefully designing co-creative interactions for stakeholder engagements
The value co-creation approach positions the source of value within the co-creation experience, which is actualised through the organisation–stakeholder or end user co-creative interactions. These interactions must be purposefully designed by strategically aligning people, processes and interfaces to co-create the value propositions and outcomes together17,29 while being mindful of stakeholders’ individual domains of experience and with the aim of building effective connections. Engagement platforms can be formal face-to-face meetings, online interactions (website, webinars, and blogs), private or public community forums, site visits or open forums. These platforms must also enable new experiences by ensuring opportunities for end users to co-create their own unique outcomes (products, services, and experiences).17,29
4. Expanding the circle of stakeholders and joint value creation opportunities
A co-creative enterprise must be cognisant of maximising the ecosystems of capabilities in the social, business, civic, and natural communities in which stakeholders exist to produce new co-creative capacities of value creation.17 It is important for the enterprise to assess value in order to verify that those involved have generated new value. Further to this, it is imperative to recognise that value is subjective and varies as a function of the co-creation experiences of stakeholders, both their experiences in interacting through the platform and the experiences of the co-created outcomes.17,29 There are many different kinds of value — economic or societal gains, organisational improvement, personal achievements, satisfied stakeholders just to name a few.17
5Engaging stakeholders in private, public, and social sectors to expand benefit for all
It is important for an enterprise to be mindful that building ecosystems of capabilities together with other private, public, and social sector enterprises will expand the wealth–welfare–wellbeing all around. By strategically engaging stakeholders across the numerous industries and domains, co-creation enables more resourceful and sustainable growth opportunities which, in turn, benefit the stakeholders in the ecosystems, the economy and society as a whole.17,26
6Deepening the impact and enable the viral spread of “win more–win more” value creation
In the co-creation paradigm, we work with others to continuously multiply and join the capabilities that exist across a variety of industries and business domains; across the private, public and social sectors. Succeeding together in growing value of many kinds, fuels a “win more–win more” environment, in which the number and scope of interested co-creation partners expands and the capability to spread and build on value co-creation approaches increases.17,26
Co-created outcomes of value
Embedding value co-creation across the CRE research program led to co-created outcomes of significant value which are described briefly below.
Robust and enduring partnerships
The approach encouraged the research team to build genuine multi-stakeholder relationships with influential partner primary care organisations, national and international researchers, clinicians, government, consumers, and relevant stakeholders to undertake collaborative research. From inception, the approach brought together influential primary care peak bodies including the Royal Australian College of General Practitioners; the Australian Association of Practice Managers; the Australian Primary Health Care Nurses Association; the Department of Health; Australian General Practice Accreditation Limited; the Improvement Foundation; Chronic Illness Alliance; and the Australian Commission on Safety and Quality in Health Care; and the Medicare Locals (now Primary Health Networks [PHNs]). These partner organisations collectively represent 40 000 primary care clinicians and managers delivering more than 100 million patient consultations per year, and organisations responsible for establishing policy, and the quality and safety benchmarks for Australian primary care.
Co-created research outcomes of value to end users
The involvement and input from the strategic partners throughout the entire research journey, that is, from the development of the research program to the implementation and evaluation phases, ensured that the co-created research outcomes were highly relevant and easily transferrable to the real world. One example of a co-created research journey is provided in Box 3, showing how value co-creation resulted in development of the Primary Care Practice Improvement Tool (PC-PIT), an on-the-ground quality improvement tool now embedded in practices Australia-wide. Another approach delivered a best-practice governance framework30 now in use in integrated care arrangements between PHNs and local hospital and health services.
Establishment of the International Implementation Research Network in Primary Care
Through co-creative networking and a focus on building value in service innovation internationally, the CRE and stakeholders began the International Implementation Research Network in Primary Care (IIRNPC). This collaboration of researchers and stakeholders shared a vision of advancing the field of implementation research with a specific focus on care transformation policy and practice.31 The IIRNPC, through multiple channels and interactions (such as e-newsletters, online forums, website interactions, a shared repository of publications and resources, and annual face-to-face meetings), stayed engaged, shared implementation research, developed expertise on implementation and translational research methods, and developed international collaborative primary care research.
Formation of the International Primary Health Reform Conference
The CRE’s approach in working with end users to co-create value in primary care research has expanded its national and international relationships and networks with influential partners. The CRE has been fortunate to co-host three successful International Primary Health Care Reform Conferences, bringing together primary care organisations, policy makers, consumers, researchers and clinicians, to continue the reform platform for primary care globally, and to further develop our international network for future growth.32
Strategies to achieve value co-creation in primary care services research
Leading theorists predict that value co-creation will become a primary source of an organisation’s competitive advantage.33 In our experience, value co-creation has drawn together strategic primary care organisations responsible for over 100 million consultations annually. As the case study (Box 3) illustrates, the key benefits of value co-creation lie in the development of relationships with stakeholders through meaningful engagement (co-creative interactions). It focuses on improving the experiences of stakeholders through the provision of strategic value creation opportunities. We propose that applying the principles of value co-creation in a way that strategically and genuinely considers all influential stakeholders from different ecosystems, maximises the productivity, creativity, utility and impact of the evidenced-based research outcomes and their translation to primary care policy and practice. To use this approach in primary care services research will require a commitment from the research enterprise to the value co-creation principles. It also requires creative research management processes and solutions and an effective leadership and governance framework.
The use and implementation of value co-creation will vary from one case to the next. Yet, there are key principles and strategies which are essential to successful value co-creation that leaders should consider as they follow the six steps and apply this approach in primary care services research. In Box 4, we provide these based on our experience of applying value co-creation. Underpinning these principles are four key lessons we learned, summarised below.
Partnership development requires an investment of time, effort and resources
The regular engagements required for research stakeholders to build effective long term relationships and co-create value takes effort, time and resources.19 Considering that most research programs or projects have limited time frames and funding, researchers must strategically factor in extended time, resources and budget to allow for successful value co-creation. In addition, funding bodies and university organisations continue to hold traditional views of research which require clearly articulated aims, set methodological processes and proposed outcomes that are largely inflexible and do not allow for the dynamic and evolving nature of value co-creation.
Management systems need to be “co-creative”
Creative research management solutions are needed to ensure that the benefits of a true co-creation approach can be achieved. This includes effective leadership and governance to manage multi-stakeholder relationships, and the design of appropriate platforms of engagement to yield useful co-created research outcomes. Traditional research teams do not typically have these skills, and may consider recruiting appropriate staff or providing training in the principles and application of the co-creation paradigm.
From the health system perspective, co-creative leadership entails the ability to embed a co-creation culture within the research enterprise, understanding the process of co-creation through its key building blocks (dialogue, access, risk assessment and transparency),34 embracing co-creative engagement, and designing co-creative management systems and processes with internal and external stakeholders.17 The research enterprise, as the organising agency, sets the overall strategic direction and defines the boundaries between what can and cannot be created.28 The governance structures, including the identification of the roles and responsibilities of people and projects, must be co-created by all involved. Research committees and boards must have representation from all stakeholders and end users of the research, and the management system should allow stakeholders to participate as co-creators throughout the entire enterprise (ie, co-creating value identification, strategy formulation and execution, fine tuning processes, involvement in problem solving, performance and risk management activities, and implementation).17
Openness and understanding is needed to work across different sectors and cultures
Working across the research–policy interface and care delivery systems can pose challenges related to differing cultures, priorities, preferred styles of communication, and time frames.23 The value co-creation approach must allow time for getting to understand stakeholder needs and values (which are subjective and can evolve in the course of the research journey) and thus ensure that the research team is in a position to better meet them (eg, designing more appropriate platforms of engagement, adjusting methods or deliverables, and producing co-created outcomes in a timely manner).
Flexibility, fairness and transparency is essential in value co-creation
It is widely accepted that value co-creation involves the free exchange of knowledge, information and contribution in different forms from external stakeholders. Therefore, issues of fairness, ethics, and intellectual property need to be considered, and in some senses reinvented, as part of an ongoing co-creation process. Once again, it is linked to a deeper understanding of stakeholder motives for involvement and engagement which can range from intrinsic (altruistic, free-worker) to extrinsic (economic rewards);35 and their perspectives of fairness, ethics, and values.36 From our experience, and supported by the literature,36 transparency and constant dialogue are the best solutions to ensure that these differing perspectives align. Clarifying expectations between stakeholders reduces potential perceptions of “free riding”, exploitation, or the perception that intellectual property is being used for the exclusive benefits of other participants or organisations. It includes mutually constructing rules of engagement, encouraging stakeholders to voice their needs, discuss their obligations, give their consent and identify perceived benefits as these evolve throughout the journey.
Conclusion
The value co-creation paradigm provides an effective framework to join researchers and the broader community in better creating end user value.23 It is an effective, sustainable approach to building and expanding long term research partnerships across multiple sectors, and increasing research productivity and the benefits of co-created outcomes for stakeholders, the health care economy and society as a whole.
As the example of the PC-PIT shows, the essence of the value co-creation is the development of long term, trusting relationships with and between key stakeholders and end users of the research, ultimately resulting in greater uptake of research outcomes into both policy and practice. This facilitates a shift in focus from traditional research processes and outcomes toward stakeholder or end user articulated processes and co-created outcomes. The “human experience”, forms the central focus of the co-creation strategy, leading to a cycle of ongoing, valuable and sustained relationships between researchers and end users.
Box 1 – Traditional strategy versus a co-creative strategy in primary care services research*
Traditional research |
Co-creative strategy |
||||||||||||||
Value: Creates value by delivering defined outcomes to targeted research end users |
Value: Creates value by constantly enhancing experiences for all stakeholders, so they remain engaged and involved in the co-creation of research outcomes |
||||||||||||||
Goals: Establishes strategic goals at the outset and does not significantly change them |
Goals: Uses the initial strategic goal as a starting point and lets the full strategy emerge over time (ie, be co-created with all stakeholders) |
||||||||||||||
Key focus: Focuses on the interests of the research organisation or team and how the they can maximise their share or gains of the outcomes relative to the shares or gains of its research competitors and the other members of its value chain |
Key focus: Focuses on the interests of all stakeholders and how the ecosystems can maximise the size of the pie; maximise the share of value captured by the research organisation as secondary |
||||||||||||||
Advantages: Achieves advantage through completing research on time and within budget, and by publishing research in academic journals and obtaining further funding to do more research |
Advantages: Achieves advantage through increased engagement of stakeholders and by continually building new interactions and experiences. These lead to co-created outcomes of value for all involved and ultimately increase uptake of research to inform policy and practice |
||||||||||||||
* Adapted from Ramaswamy and Gouillart.28 | |||||||||||||||
Box 2 – Value co-creation in primary care services research*
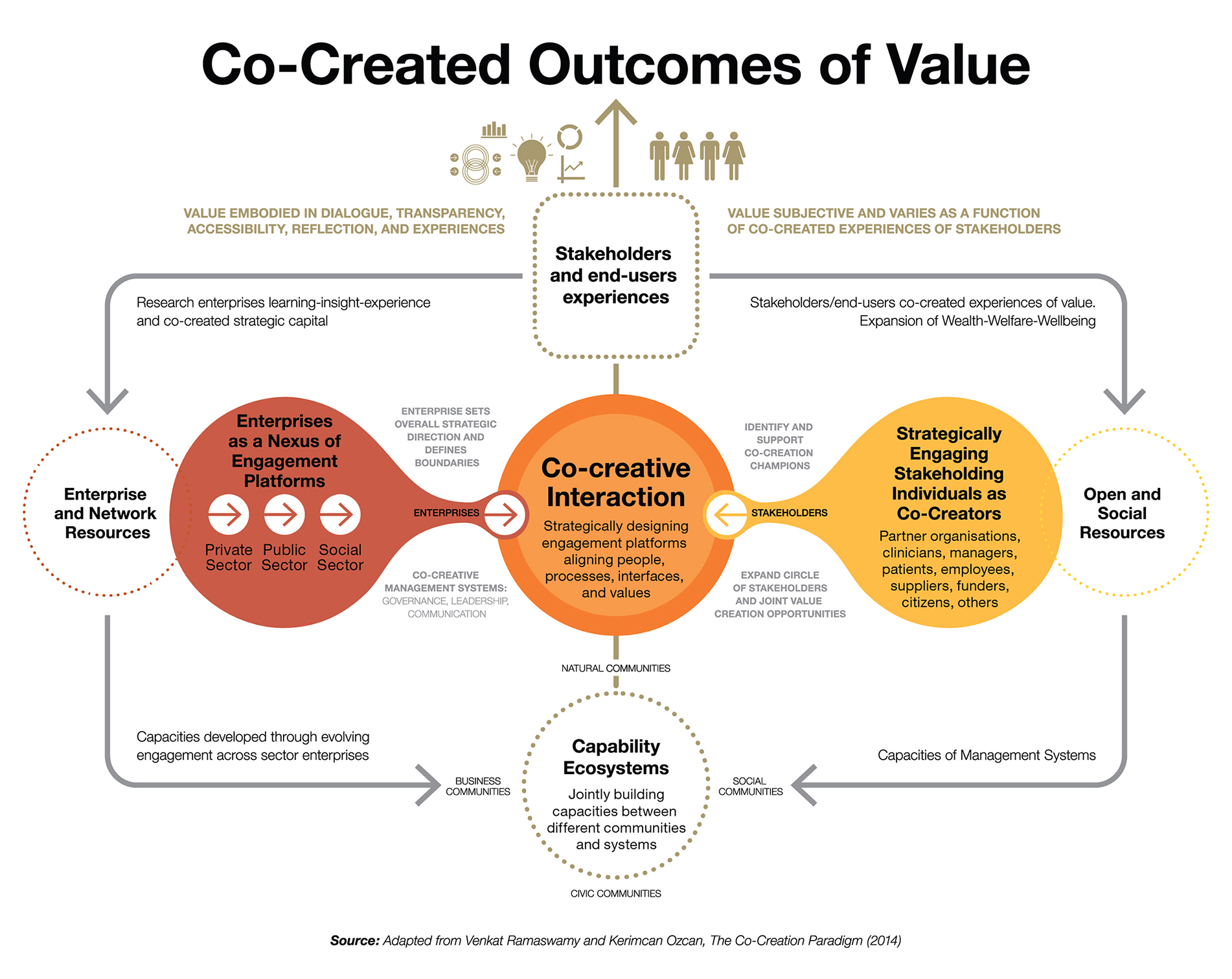
Adapted from Ramaswamy and Ozcan, 2014, figures 1–3, page 29.17
Box 3 – Case study: the development and trial of the Primary Care Practice Improvement Tool (PC-PIT)*
Steps |
Description |
||||||||||||||
Strategically engaging varying stakeholders in creating value together |
Partners included primary care peak bodies, the federal Department of Health, primary care clinicians and managers, Medicare Locals (quality improvement and practice support units), GPs (clinical leaders) and practice managers (organisational leaders) providing strategic input into the application of the tool. Initial implementation and evaluation of a pre-existing organisational improvement tool revealed extensive problems, namely jargonistic language; a complex and lengthy implementation process and the need for ongoing, expert external facilitation. Thus, a new, co-created aim was developed to co-design and trial a tool bespoke for Australian general practice. |
||||||||||||||
Identifying and supporting champions |
Champions included practice managers and practice nurses as well as principal GPs. Participants provided a strategic link to their organisational values and expectations. Trusting relationships developed across previously disparate groups. The research team was thus able to tie the research process back to strategic enterprises, for example, the design and implementation of the PC-PIT linked to the role, education and support for practice managers in organisational performance improvement. |
||||||||||||||
Purposefully designing platforms (or co-creative interactions) for stakeholder engagements |
Engagement platforms included formal partner meetings, one-on-one in-depth discussions, combined partner and stakeholder feedback sessions (formal presentations), end user advisory committees, teleconferences, social (online) and printed (newsletters) media. Stakeholders identified a list of desired attributes an improvement tool should encompass, along with a shared vision for a “one stop shop” of organisational improvement resources mapped to existing quality improvement programs.† |
||||||||||||||
Expanding the circle of stakeholders and joint value creation opportunities |
All stakeholding individuals were able to influence processes and outcomes and be involved in collective problem solving. Increased trust led to data and resource sharing, creating new capacities and expediting strategic decisions. Focus on the role of practice managers as organisational leaders and practice nurses as facilitators of organisational development created a sense of satisfaction in these professional groups and a sense of ownership in relation to performance improvement programs. Medicare Locals and the Primary Health Networks ensured the PC-PIT could be embedded into existing quality improvement frameworks. The Department of Health ensured the PC-PIT was in line with system policies relating to practice performance incentives. |
||||||||||||||
* Appendix 1 provides an illustration of PC-PIT co-creation. † Appendix 2 has additional information about engagement platforms developed for co-creating the PC-PIT. | |||||||||||||||

Provenance: Commissioned; externally peer reviewed.
- Tina Janamian
- Lisa Crossland
- Claire L Jackson
- Discipline of General Practice, Centre of Research Excellence – Building Primary Care Quality, Performance and Sustainability via Research Co-Creation, University of Queensland, Brisbane, QLD
The research reported in this article is a project of the Australian Primary Health Care Research Institute (APHCRI), which is supported by a grant from the Australian Government Department of Health. The information and opinions contained in it do not necessarily reflect the views or policy of the APHCRI, the Australian Government, or the Department.
No relevant disclosures.
- 1. Armstrong K, Kendall E. Translating knowledge into practice and policy: the role of knowledge networks in primary health care. Health Inform Manage J 2010; 39: 9-17.
- 2. Crabtree BF, Nutting PA, Miller WL, et al. Primary care practice transformation is hard work: insights from a 15-year developmental program of research. Med Care 2011; 49: S28-35.
- 3. Lomas J. Using research to inform healthcare managers’ and policy makers’ questions: from summative to interpretive synthesis. Healthcare Policy 2005; 1: 55-71.
- 4. Ornstein S, Nietert PJ, Jenkins RG, et al. Improving the translation of research into primary care practice: results of a national quality improvement demonstration project. Jt Comm J Qual Patient Saf 2008; 34: 379-390.
- 5. van Weel C. Primary-care research to inform policy and implementation. Lancet 2013; 382: 1156-1157.
- 6. Jackson CL, Janamian T, van Weel C, et al. Implementation research — its importance and application in primary care. Med J Aust 2014; 201 (3 Suppl): S42-S43. <MJA full text>
- 7. Jackson CL, Greenhalgh T. Co-creation: a new approach to optimising research impact? Med J Aust 2015; 203: 283-284. <MJA full text>
- 8. McKeon S, Alexander E, Brodaty H, et al. Strategic review of health and medical research. Better health through research. Canberra: Australian Government Department of Health and Ageing, 2013.
- 9. Frank C, Nason E. Health research: measuring the social, health and economic benefits. CMAJ 2009; 180: 528-534.
- 10. Bouter LM. Knowledge as a common good: the societal relevance of scientific research. Higher Educ Manage Policy 2010; 22: 119-132.
- 11. Thorp H, Goldstein B. Engines of innovation: the entrepreneurial university in the twenty-first century: Chapel Hill, NC: University of North Carolina Press, 2013.
- 12. Green LW. Making research relevant: if it is an evidence-based practice, where’s the practice-based evidence? Fam Prac 2008; 25 Suppl 1: i20-i24.
- 13. Peters DH, Adam T, Alonge O, et al. Implementation research: what it is and how to do it. BMJ 2013; 347: f6753.
- 14. Schmittdiel JA, Grumbach K, Selby JV. System-based participatory research in health care: an approach for sustainable translational research and quality improvement. Ann Fam Med 2010; 8: 256-259.
- 15. Clancy CM, Slutsky JR, Patton LT. Evidence-based health care 2004: AHRQ moves research to translation and implementation. Health Serv Res 2004; 39: xv-xxiii.
- 16. Woolf SH. The meaning of translational research and why it matters. JAMA 2008; 299: 211-213.
- 17. Ramaswamy V, Ozcan K. The co-creation paradigm. Stanford, Calif: Stanford University Press; 2014.
- 18. Gouillart F, Hallett T. Co-creation in government. Stanford Soc Innovat Rev 2015; Spring.
- 19. McColl-Kennedy J. Health care in service science special issue of Australasian Marketing Journal. Aust Mark J 2014; 22: 165-167.
- 20. McColl-Kennedy J, Vargo S, Dagger T, et al. Healthcare customer value co-creation practice styles. J Service Res 2012; 15: 370-389.
- 21. Merz M, Czerwinski D, Merz MA. Exploring the antecedents for value co-creation during healthcare service provision. J Bus Behav Sci 2013; 24: 152-156.
- 22. Janamian T, Crossland C, Wells L. On the road to value co-creation in health care: the role of consumers in defining the destination, planning the journey and sharing the drive. Med J Aust 2016; 204 (7 Suppl): S12-S14.
- 23. Janamian T, Jackson CL, Dunbar JA. Co-creating value in research: stakeholders’ perspectives. Med J Aust 2014; 201 (3 Suppl): S44-S46. <MJA full text>
- 24. Ramaswamy V, Gouillart F. The power of co-creation: build it with them to boost growth, productivity, and profits. New York: Free Press, 2010.
- 25. Hearn G, Pace C. Value-creating ecologies: understanding next generation business systems. Foresight 2006; 8: 55-65.
- 26. Randall R, Leavy B. Venkat Ramaswamy — how value co-creation with stakeholders is transformative for producers, consumers and society. Strategy Leadership 2014; 42: 9-16.
- 27. Normann R, Ramirez R. Designing interactive strategy. Harvard Bus Rev 1993; July-August.
- 28. Ramaswamy V, Gouillart F. Building the co-creative enterprise. Harvard Bus Rev 2010; 88: 100-109.
- 29. Ramaswamy V, Chopra N. Building a culture of co-creation at Mahindra. Strategy Leadership 2014; 42: 12-18.
- 30. Nicholson C, Jackson CL, Marley J. Best-practice integrated health care governance — applying evidence to Australia’s health reform agenda. Med J Aust 2014; 201 (3 Suppl): S64-S66. <MJA full text>
- 31. International Implementation Research Network in Primary Care. About the IIRNPC [website]. http://iirnpc.net/?page_id=8 (accessed Jan 2016).
- 32. International Primary Health Care Reform Conference. Creating value: but for whom. 3rd International Primary Health Reform Conference; 14–16 Mar 2016. Brisbane: IPHCRC. http://yrd.com.au/IPHCRC16_Program_071215.pdf (accessed Jan 2016).
- 33. Gouillart FJ. The race to implement co-creation of value with stakeholders: five approaches to competitive advantage. Strategy Leadership 2014; 42: 2-8.
- 34. Prahalad CK, Ramaswamy V. Co-creating unique value with customers. Strategy Leadership 2004; 32: 4-9.
- 35. Zwass V. Co-creation: toward a taxonomy and an integrated research perspective. Int J Elect Commerce 2010; 15: 11-48.
- 36. Windisch K. Co-creation and the ethics of stakeholder engagement for value creation. Denmark: Arhus University; 2011.
Summary