




Using mobile phones to acquire images in clinical practice enables rapid, collaborative decision making1 and is increasingly common. However, the practice is not completely foolproof, as a recent “near miss” at our institution demonstrates.
A 45-year-old woman presented with spontaneous subarachnoid haemorrhage secondary to a ruptured anterior communicating artery aneurysm. The anterior communicating artery aneurysm and an unruptured left middle cerebral artery aneurysm were clipped via craniotomy and a ventricular drain was inserted. Serial post-operative computed tomography (CT) brain scans showed an evolving infarction in the left middle cerebral artery territory, presumed to be secondary to temporary clipping at surgery, which became fully established after 28 hours. All cerebral vessels were patent, visualised on a post-operative CT angiogram. Elevated intracranial pressure (> 40 mmHg) and neurological fluctuation prompted a repeat CT scan, a photograph of which was taken from a computer screen using a mobile phone (Box, A). This image was sent by the intensive care unit consultant to the mobile phone of the on-call neurosurgeon, who noted apparent extensive bifrontal infarction. The patient was urgently transported to the operating room for decompressive craniectomy; however, on reviewing the scans at a radiology workstation before surgery (Box, B), the neurosurgeon noted the discrepancy and the procedure was cancelled. The patient recovered well and was neurologically intact and independent 6 months after discharge.
Although others report success using mobile phones to photograph CT brain scans displayed on computer monitors,2 our case highlights the need for doctors to appreciate the limitations of display technology. For example, many computer monitors exhibit viewing angle-dependent reductions in luminance and contrast ratio,3 which render images susceptible to artefact, particularly when viewed at close range.4 Moreover, mobile phone screens do not meet the technical requirements of a medical imaging display device.5
We confirmed that viewing angle-dependent reductions in luminance were responsible for the spurious frontal lobe darkening evident in the mobile phone image. Clearly, spatial variations in image brightness can dramatically affect image interpretation, with potentially disastrous results.
Guidelines on mobile device photography in the health care setting address privacy concerns but not technical aspects.1 Therefore, we offer some suggestions on preventing similar cases from occurring:
Use original images wherever possible.
Compare the photo with the original before sending.
When photographing computer screens, position the camera perpendicularly to, and at arm’s length from the screen, enlarging the image with digital zoom as required.
Before making clinical decisions, review the original imaging, including confirming the correct patient details with an observer or peer.
After photographing, ensure that images are deleted from the phone and any online data storage accounts, and record in writing the image use in the case notes.
Teach undergraduates as well as practising clinicians the technical aspects of the use of mobile phone images.
We hope this case serves to remind doctors of the need for caution when reviewing photographs of digital images, and that our suggestions will be helpful in preventing similar situations from occurring.
Box – Mobile phone photograph of the cranial computed tomography (CT) scan compared with the original image
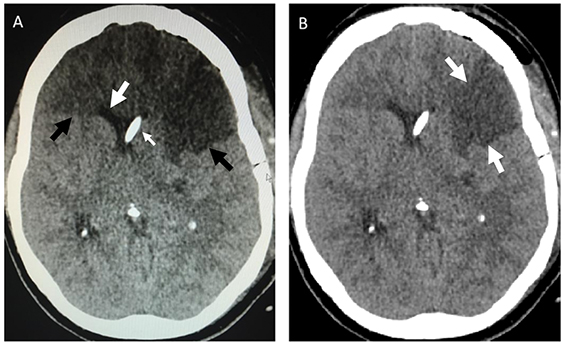
A: Photograph of axial CT image sent via a mobile phone, showing apparent hypodense frontal lobes suggestive of infarction (black arrows). Note however the anterior horns of the lateral ventricles are not distorted or effaced, as would be expected with such an extensive infarct (large white arrow). A ventricular catheter is located in the right lateral ventricle (small white arrow). B: The original axial CT image showing only a wedge-shaped, left middle cerebral artery infarct (white arrows).
Received 31 August 2015, accepted 16 November 2015
- Jarrel Seah1
- Andrew D Nichols2
- Philip M Lewis1,2
- Jeffrey V Rosenfeld1,2
- 1 Monash University, Melbourne, VIC
- 2 Alfred Hospital, Melbourne, VIC
No relevant disclosures.
- 1. Australian Medical Association. Clinical images and the use of personal mobile devices: a guide for medical students and doctors. 2015. https://ama.com.au/article/clinical-images-and-use-personal-mobile-devices (accessed Aug 2015).
- 2. Bullard TB, Rosenberg MS, Ladde J, et al. Digital images taken with a mobile phone can assist in the triage of neurosurgical patients to a level 1 trauma centre. J Telemed Telecare 2013; 19: 80-83.
- 3. Badano A, Flynn MJ, Martin S, Kanicki J. Angular dependence of the luminance and contrast in medical monochrome liquid crystal displays. Med Phys 2003; 30: 2602-2613.
- 4. Ghodrati M, Morris AP, Price NS. The (un)suitability of modern liquid crystal displays (LCDs) for vision research. Front Psychol 2015; 6: 303.
- 5. Yamazaki A, Liu P, Cheng WC, Badano A. Image quality characteristics of handheld display devices for medical imaging. PLoS One 2013; 8: e79243.
Trevor Kwok
In the situation described, the referring doctor could have sent a high-quality screenshot of the CT image to the surgeon through internal email, which the surgeon could have accessed remotely and securely, avoiding issues of both image quality and legality/privacy.
I would be interested to know whether the change in luminance due to the viewing angle of the photographer was the sole factor causing the difference between the original CT image and the photograph. Could other factors, such as ambient lighting and automatic image processing by the mobile phone, have played a role in causing the problem?
In public hospital vascular surgery practice, it is common for junior doctors to send photographs of wounds (often diabetic foot ulcers or previously debrided wounds) to senior colleagues, who are often busy in theatre, for appraisal. Inconsistences in lighting and white balance have been identified as caveats of clinical photography with mobile phones.[1] One study showed that among surgeons assessing mobile phone photographs of wounds, the presence of tissue necrosis was misdiagnosed in 21% of cases.[2] It is borne out by personal experience that such photographs often give a false clinical impression, and decisions on discharge from hospital, and the need for surgical debridement, based on these photographs are likely to be wrong.
While the potential benefits of mobile phone photography as part of telemedicine for isolated remote patients are obvious, its use in the contexts discussed here, within metropolitan hospitals, needs much better understanding and should be regarded with caution.
References
1. Ashique KT, Kaliyadan F, Aurangabadkar SJ. Clinical photography in dermatology using smartphones: an overview. Indian Dermatol Online J 2015; 6: 158-63.
2. Chen CH, Young TH, Huang CH, Chang HH, Chen CL, Chien HF, et al. Patient-centered wound teleconsultation for cutaneous wounds: a feasibility study. Ann Plast Surg 2014; 72: 220-4.
Competing Interests: No relevant disclosures
Dr Trevor Kwok
St Vincent's Hospital, Sydney, NSW