




Prothrombinex-VF powder for injection (PTX-VF; CSL Biotherapies, Melbourne, Vic) is a prothrombin complex concentrate (PCC). Each vial contains 500 IU factor II, 500 IU factor IX, 500 IU factor X, 25 IU antithrombin III, 192 IU heparin sodium and ≤ 500 mg human plasma proteins. PTX-VF is indicated in the treatment and perioperative prophylaxis of bleeding in acquired deficiency of coagulation factors caused by vitamin K antagonists (ie, warfarin), and the treatment and prophylaxis of bleeding in patients with congenital coagulation factor deficiency. However, clinical data on the efficacy of PTX-VF are limited and the optimal dose is yet to be determined.1-3 Locally, the Australasian Society of Thrombosis and Haemostasis Warfarin Reversal Consensus Group recommends 25–50 IU/kg of PTX-VF combined with fresh frozen plasma (FFP) or vitamin K.4 However, previous audits suggest that relatively low doses effectively reduce international normalised ratio (INR), even without FFP.5
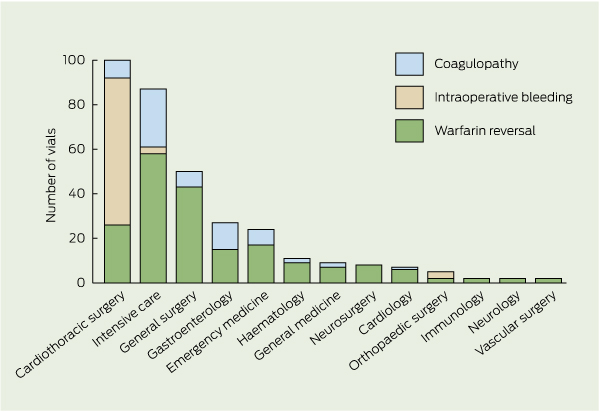
Indications for PTX-VF fell into three groups: warfarin reversal, intraoperative bleeding, and coagulopathy (prolonged INR [greater than 1.5] not due to warfarin). Some patients had overlapping indications and multiple medical teams involved in their care, therefore the predominant indication was used for our analyses (Box 1). The numbers of vials prescribed by specialty and indication are shown in Box 2.
The contribution of FFP for warfarin reversal was examined by comparing prescriptions of PTX-VF given with and without FFP (Box 3). A median of two units of FFP was given in the PTX-VF with FFP group and the number of patients prescribed vitamin K was not significantly different between groups (P = 0.15; odds ratio, 0.49 [95% CI, 0.18 to 1.3]). There was a significant decrease in INR over time that was independent of group (P < 0.001; 95% CI, 0.3 to 0.4). There was a significant difference in the rate of change in INR between groups (P = 0.008; 95% CI, − 0.2 to − 0.1), with the PTX-VF alone group decreasing by a smaller amount, although this group also had a smaller mean dose of PTX-VF (P = 0.007).
Lower doses of PTX-VF (< 25 IU/kg) were compared with higher doses (25–50 IU/kg) for warfarin reversal (Box 4). There was a significant difference in mean PTX-VF dose between the groups (16.1 IU/kg in lower-dose group v 29.1 IU/kg in higher-dose group; P < 0.001). No significant difference was found between groups for the number of FFP units or the number of vitamin K prescriptions. There was a significant decrease in INR over time that was independent of group (P = 0.002; 95% CI, − 3.1 to − 0.7). There was no evidence of a difference in the rate of change in INR between groups (P = 0.56; 95% CI, − 0.8 to 1.6).
Seventy-two vials of PTX-VF were given for intraoperative bleeding over 20 prescriptions (Box 1), mainly during cardiothoracic surgery (Box 2) — most commonly during heart valve replacements and heart transplantation. No patients in this group had been treated with warfarin. The mean PTX-VF dose in this group was 23.0 IU/kg (95% CI, 18.6 to 28.4 IU/kg), and mean INR was unchanged over time (less than 1.5 before and after treatment). Haemostatic agents given concurrently included platelets (15 of 20 prescriptions), FFP (12), protamine (seven), tranexamic acid (six), vitamin K (one) and factor VIIa (one). PTX-VF was prescribed as first-line therapy for intraoperative bleeding for seven prescriptions, as second-line therapy for five prescriptions, and third-line for the remaining prescriptions. Haemostasis was achieved in all cases. Factors contributing to intraoperative bleeding included thrombocytopenia (six cases) and prolonged APTT (seven cases).
Twenty-one prescriptions of PTX-VF were for coagulopathy that was not due to warfarin but was secondary to liver synthetic dysfunction, shock or multiorgan failure — 13 prescriptions for active bleeding and eight for impending procedures. The mean PTX-VF dose was 16.8 IU/kg (95% CI, 12.9 to 21.9 IU/kg) and other haemostatic agents given are shown in Box 1. The mean INR decreased from 2.2 (95% CI, 1.9 to 2.6) to 1.7 (95% CI, 1.4 to 1.9) overall. Haemostasis was achieved with haemostatic agents in 9 of the 13 patients with active bleeding; the others required surgical intervention. Those with an impending procedure were given PTX-VF before the procedure, which reduced INR in all cases.
Interactions with tranexamic acid have been reported, and six patients were given tranexamic acid with PTX-VF (20.0–41.7 IU/kg) during cardiothoracic surgery for haemostasis; five had no complications and the other died from an unrelated cause. Monitoring of factor IX levels was not performed. Fourteen patients died within 7 days of PTX-VF therapy, but these deaths were unrelated to PTX-VF (six patients had organ failure, four had sepsis, three had malignancy and one had multiple trauma).
Warfarin is commonly used for treatment of atrial fibrillation and thromboembolic disease and for stroke prevention, and the number of patients prescribed warfarin in Australia is expected to increase due to the ageing population.6 Safe warfarin reversal is therefore important to permit surgery and treat major bleeding (major bleeding affects about 6.5% of patients anticoagulated with warfarin annually, and about 1% of such bleeds are fatal).7
We found that PTX-VF is effective for warfarin reversal without FFP, which is consistent with results of previous studies.3,5-7 FFP and some four-factor PCCs1,2,8 contain large amounts of factor VII, while PTX-VF and other three-factor PCCs contain little to no factor VII. We therefore believe that factor VII is not important for warfarin reversal, as this can be achieved with PTX-VF and other three-factor PCCs.4-6,9 Recent guidelines from the British Committee for Standards in Haematology recommend that FFP should only be used for major bleeding when PCCs are not available.3 Advantages of PTX-VF (and other PCCs) over FFP include immediate onset of action, easier storage, easier reconstitution without time needed to thaw, less risk of disease transmission, and no risk of transfusion-related lung injury, fluid overload or blood group incompatibility.4-7,9 Also, reintroduction of warfarin after surgery to return to a stable anticoagulated state has been successfully shown in patients given PTX-VF.9
Lower doses of PTX-VF (< 25 IU/kg) are effective for warfarin reversal. We found significant INR reduction independent of lower-dose or higher-dose group with similar doses of vitamin K and FFP. Ex-vivo testing of reduction of INR values greater than 4 with one dose (500 IU) of PCC has been found to normalise INR.2 However, we cannot recommend that this finding be extrapolated to patients who have an INR value greater than 4 because there were few such patients in our study — most had a pretreatment INR between 2.0 and 3.0.
Adherence to guidelines4 was poor in our audit. There were large variations in dose (in IU/kg) and PTX-VF usage in bleeding patients who had normal coagulation profiles before administration of PTX-VF and other blood products. Despite divergence from the warfarin reversal consensus guidelines, the INR reduction to 1.5 or less in most (40 of 66) prescriptions and cessation of bleeding in most cases supports lowering the recommended PTX-VF dose in future revisions of guidelines. When INR did not reduce to 1.5 or less, haemodynamic instability or sepsis was present in most cases.
Use of PCCs in intraoperative bleeding (an indication for which it is not licensed) is emerging. In 2008, a retrospective analysis of the role of PCCs in bleeding surgical patients whose condition had not responded to conventional blood products demonstrated the potential value of PCCs in controlling bleeding during surgery after standard blood products had failed.8 In our audit, 66 vials of PTX-VF were prescribed for intraoperative bleeding during cardiothoracic surgery, possibly because of the results of the abovementioned analysis and for its perceived superiority over FFP in thrombin augmentation and subsequent effects on platelet activation. As blood loss was not accurately quantified, plasma factor levels were not checked and the timing of PTX-VF among other blood products varied, conclusions cannot be made about use of PTX-VF in intraoperative bleeding from our data. A prospective study is currently running at RPH to assess whether PTX-VF significantly decreases blood transfusion requirements in cases of intraoperative bleeding.
1 Patient characteristics, PTX-VF treatment details and results of laboratory testing by treatment group
Received 21 June 2011, accepted 2 November 2011
- Paul C Kruger1
- Annette S Le Viellez2
- Richard P Herrmann2
- 1 Department of Haematology, Fremantle Hospital and Health Service, Fremantle, WA.
- 2 Haematology Department, Royal Perth Hospital, Perth, WA.
We thank Sally Burrows (Biostatistician, School of Medicine and Pharmacology, University of Western Australia and RPH) for performing the data analysis.
No relevant disclosures.
- 1. Junagade P, Grace R, Gover P. Fixed dose prothrombin complex concentrate for the reversal of oral anticoagulation therapy. Hematology 2007; 12: 439-440.
- 2. Gatt A, Riddell A, van Veen JJ, et al. Optimizing warfarin reversal – an ex vivo study. J Thromb Haemost 2009; 7: 1123-1127.
- 3. Evans SJ, Biss TT, Wells RH, Hanley JP. Emergency warfarin reversal with prothrombin complex concentrates: UK wide study. Br J Haematol 2008; 141: 268-269.
- 4. Baker RI, Coughlin PB, Gallus AS, et al; Warfarin Reversal Consensus Group. Warfarin reversal: consensus guidelines, on behalf of the Australasian Society of Thrombosis and Haemostasis. Med J Aust 2004; 181: 492-497. <MJA full text>
- 5. Crawford JH, Augustson BM. Prothrombinex use for the reversal of warfarin: is fresh frozen plasma needed? Med J Aust 2006; 184: 365-366. <MJA full text>
- 6. Tran H, Collecutt M, Whitehead S, Salem HH. Prothrombin complex concentrates used alone in urgent reversal of warfarin anticoagulation. Intern Med J 2011; 41: 337-343.
- 7. Leissinger CA, Blatt PM, Hoots WK, Ewenstein B. Role of prothrombin complex concentrates in reversing warfarin anticoagulation: a review of the literature. Am J Hematol 2008; 83: 137-143.
- 8. Bruce D, Nokes TJ. Prothrombin complex concentrate (Beriplex P/N) in severe bleeding: experience in a large tertiary hospital. Crit Care 2008; 12: R105.
- 9. Chiu D, Grigg M, Levi E. Operating on patients with warfarin: simpler alternative approach. ANZ J Surg 2009; 79: 409-410.
Abstract
Objective: To assess the use of Prothrombinex-VF powder for injection (PTX-VF) at Royal Perth Hospital and analyse the efficacy and safety profile of PTX-VF.
Design, setting and patients: A prospective observational audit of PTX-VF use, conducted by reviewing medical records and laboratory and imaging results for all patients prescribed PTX-VF from 1 November 2009 to 1 May 2010.
Main outcome measures: Data on indication, diagnosis, comorbidities, dose of PTX-VF, fresh frozen plasma (FFP) and vitamin K, coagulation parameters before and after PTX-VF administration, and adverse effects.
Results: 334 vials of PTX-VF were administered to 84 patients over 107 prescriptions. Indications were warfarin reversal, intraoperative bleeding and coagulopathy (66, 20 and 21 prescriptions, respectively). PTX-VF with FFP was compared with PTX-VF alone for warfarin reversal and there was a significant decrease in international normalised ratio (INR) that was independent of group (P < 0.001). Lower doses of PTX-VF (< 25 IU/kg) were compared with higher doses (25–50 IU/kg) for warfarin reversal and decrease in INR was significant, independent of group (P = 0.002). PTX-VF was administered for intraoperative bleeding in 18 patients who had not been treated with warfarin. No hypersensitivity reactions, thrombotic complications or worsening of disseminated intravascular coagulation occurred during 7-day follow-up.
Conclusion: For warfarin reversal, lower doses of PTX-VF (< 25 IU/kg) and PTX-VF without FFP were effective. PTX-VF was also used in intraoperative bleeding and non-warfarin coagulopathy. No adverse events were associated with PTX-VF.