




Emergency departments (EDs) can provoke anxiety among patients.1 There have been few trials of interventions that might reduce this anxiety. Although live performance has positive effects on patients and staff,2 incorporating live music in busy EDs is unrealistic.
Several auditory interventions can modify patients’ anxiety in hospital. The positive effect of music on anxiety has been well demonstrated. A review of 42 randomised contriolled trials found that about half of them showed that music was effective in reducing perioperative pain and anxiety.3 Reduced preoperative anxiety has also been associated with audio featuring binaural beats,4 which are apparent sounds perceived independent of physical stimuli.5 Binaural beats are perceived when two sounds of similar but slightly different frequency are presented separately to each ear and produce two apparent new frequencies — the sum and the difference of the original two sounds.5 This is an auditory brainstem response to the difference in amplitude of the original two tones. Binaural beat may induce a meditation-like state and also reduce chronic anxiety.6
Only a few studies have explored the impact of music on anxiety in the ED setting. Music therapy has been shown to alleviate anxiety among adults accompanying children to the ED,7 but not among adults undergoing laceration repair.8 One pilot study showed reduced pain9 among ED patients, and others showed some benefit on self-rated stress and noise disturbance.10,11 No study has investigated possible anxiolytic effects of sound interventions or binaural beat among adult ED patients.
Using the results of a preliminary study to determine patients’ listening preferences (Box 1), four 20-minute sound recordings were created:
electroacoustic musical composition;
sound compositions from audio field recordings of natural and constructed settings;
sound compositions from audio field recordings obtained from natural settings with embedded binaural beat;
reconstructed ambient noise simulating the ED but free of clear verbalisations.
Patients were eligible to participate if they were ≥ 18 years of age and were classified on arrival in the ED as category 3 according to the Australasian Triage Scale (ATS)13 — that is, patients with an acuity level indicating they required medical assessment within 30 minutes. Participation was restricted to these patients to maximise homogeneity in the sample. Patients were excluded if they had a hearing impairment, did not speak English or were unable to give informed consent (eg, cognitively impaired or highly care-dependent patients). No attempt was made to specifically recruit patients who were anxious.
Patients’ anxiety levels were self-reported as measured by the Spielberger State–Trait Anxiety Inventory (STAI),14 a 40-item self-report measure containing 20 items measuring state anxiety (anxiety experienced at that moment) and 20 measuring trait anxiety (usual level of anxiety). Scores for state and trait components each range from 20 to 80, with a higher score corresponding to higher anxiety. This scale is the most widely validated anxiety scale.14,15
no soundtrack intervention, headphones only (control group);
reconstructed ambient noise simulating ED noise but free of clear verbalisations;
electroacoustic musical composition;
composed non-musical audio field recordings;
combination of audio field recordings with embedded binaural beat.
This study was approved by the Human Research Ethics Committee at SVHM.
Our sample size estimate was based on previous studies investigating binaural beat and anxiety using the STAI.4,16 With power set at 90%, to detect a difference between means with a two-sided test at a 5% significance level, a sample size of 34 in each group was required (assuming a difference in means of 13% and a common standard deviation of 10%).
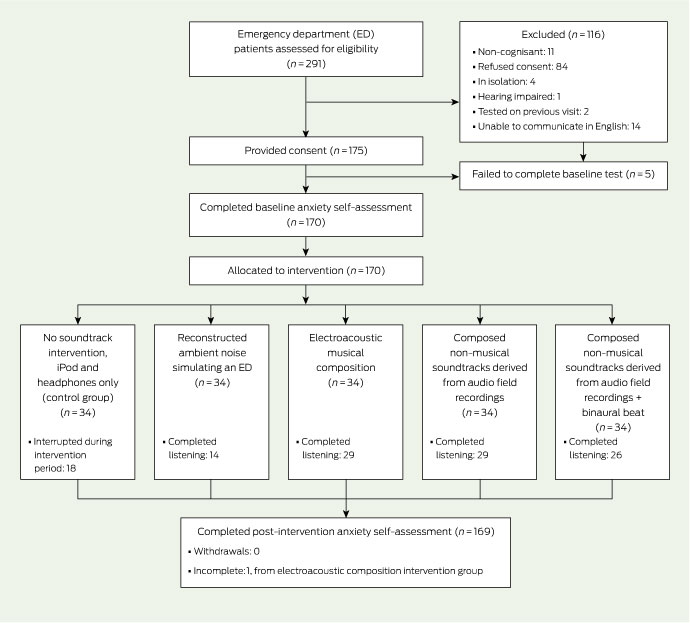
Between 1 February 2010 and 14 April 2010, 291 category 3 patients in the SVHM ED were considered for participation in our study. Of those approached, 84 refused consent, 32 were considered ineligible and 175 consented (Box 2). Five of those who consented failed to complete baseline STAI and were withdrawn. The remaining 170 participants were equally allocated to one of the five interventions (34 per group). There were no violations of allocation protocol; however, one patient did not complete the post-intervention STAI. Those refusing consent did not differ significantly from the sample in terms of age, sex, Australian country of birth, or modal presenting complaint.
The demographic characteristics of the final sample were comparable to all other patients who would have been eligible to participate based on ATS code (Box 3). Sixty-nine percent (118) of participants required pain relief during their ED stay. No significant differences were found between any groups in terms of age, sex or pain relief required. Participants had a broad range of presenting complaints (Box 4).
There was a significant interaction effect between time and intervention (F(4,164) = 6.28; P < 0.001), indicating a change over time in some, but not all, of the intervention groups. Pairwise comparison based on mean total state anxiety levels (Box 5) revealed a significant decrease in anxiety (post-intervention mean compared with pre-intervention mean) among participants listening to the electroacoustic composition (P = 0.001), composed audio field recordings (P < 0.001), and composed audio field recordings + binaural beat (P < 0.001). When compared with each other, these same three groups showed no significant difference in post-intervention mean level of anxiety.
After accounting for baseline anxiety levels, significant differences were observed between groups, with those allocated to receive the electroacoustic composition, composed audio field recordings, or composed audio field recordings + binaural beat reporting significantly lower levels of anxiety after the intervention compared with those in the control group and the group listening to simulated ED sound (Box 6). These effects were unchanged after controlling for provision of pain relief.
Our study is the first randomised controlled trial to show that sound compositions decrease anxiety in adult ED patients. We showed that the baseline level of anxiety in patients in the mid range of urgency in an Australian ED was moderate at baseline. Mean normal state anxiety scores have previously been reported as 35.7 for men and 35.2 for women.19 In our study, they ranged between 38.9 and 43.7 for the five groups, indicating moderate anxiety. Mean anxiety was significantly reduced among patients who listened to electroacoustic music, audio field recordings or audio field recordings with embedded binaural beat, to between 33.7 and 36.9 — a level of no or low anxiety. The statistically significant effect size of about 10%–15% was felt to be clinically significant as well. We did not investigate whether the effect persisted beyond the post-intervention assessment or was transient. The control group and the participants who listened to simulated ED sounds remained moderately anxious after the intervention.
A previous study using music during laceration repair in a Pittsburgh ED showed that listening was associated with reduced pain but not reduced anxiety.8 In that study, participants chose the artist and style of music. In contrast, our study used highly original compositions developed by experienced musicians and composers, and we did not record particular anxiety-provoking activities experienced by our patients, who received usual ED care and procedures for category 3 patients. Such patients are typically quite unwell and undergo many investigations and procedures. Our results indicate that these patients gained considerable relief from anxiety by listening to sound compositions and raise the possibility that such original compositions are more effective in alleviating anxiety than simply listening to well known music. This should be explored in future research.
We found that binaural beat provided no additional anxiety reduction over audio field recordings alone, in contrast with the 26% reduction in preoperative anxiety observed elsewhere.4 This raises the possibility that binaural beat is less effective in the busy ED environment than in the quiet preoperative area.
A potential limitation of this study is the use of the STAI. At a total length of 40 items (20 state, 20 trait), the length of the scale may limit its clinical utility in the ED. Although a 6-item short version of the STAI exists,20 the validity in a broad range of clinical samples was unknown at the time we began the study. Nonetheless, only five patients (2.9%) failed to complete the pre-intervention STAI.
The use of randomised controlled trial methodology precluded allowing patients to choose preferred or familiar sounds. Although sound preference and familiarity are important factors in the efficacy of sounds to relieve anxiety,4 this has not always been observed.8
1 Preliminary study
In a preliminary study,12 ten 60-second electroacoustic soundtracks, and ten 60-second composed environmental soundtracks were created. For electroacoustic soundtracks, decisions regarding the inclusion of sounds, instruments, tempo, dynamics and timbre were based on the composer’s aesthetic judgements and feedback from fellow researchers — for example, what they liked and what they found relaxing. Environmental soundtracks were created, arranged and mixed to reflect the acoustic and spatial complexities of regional and urban environments, including natural bush habitats, farms, city streets, the beach and factories.
3 Comparison of participants with all patients attending the ED during the study period and classified as category 3 on the ATS
ATS = Australasian triage scale. ED = emergency department. * 2.9% required an interpreter. |
|||||||||||||||
5 Mean total state anxiety scores before allocation and after the intervention, and number of participants requiring pain relief*
Total state anxiety, mean (SEM) |
|||||||||||||||
6 Percentage difference in mean (SEM) state anxiety compared with baseline, by intervention group
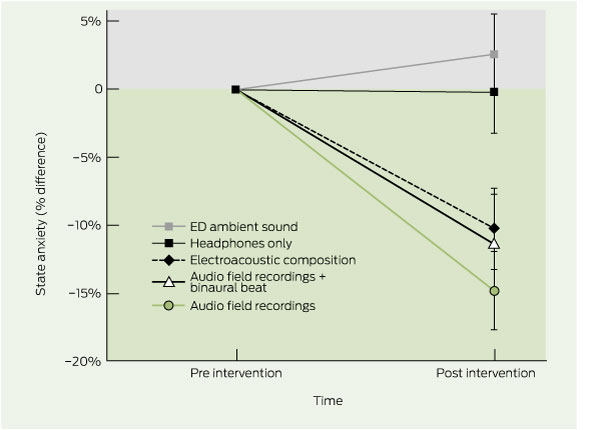 ED = emergency department. Vertical bars represent SEM. P <0.05 significant. |
Received 24 June 2010, accepted 30 November 2010
- Tracey J Weiland1
- George A Jelinek1
- Keely E Macarow3
- Philip Samartzis2
- David M Brown2
- Elizabeth M Grierson2
- Craig Winter1
- 1 Emergency Medicine, St Vincent's Hospital and University of Melbourne, Melbourne, VIC.
- 2 School of Art, RMIT University, Melbourne, VIC.
No relevant disclosures.
- 1. Ekwall A, Gerdtz M, Manias E. Anxiety as a factor influencing satisfaction with emergency department care: perspectives of accompanying persons. J Clin Nurs 2009; 18: 3489-3497.
- 2. Lelchuk Staricoff R. Arts in health: a review of the medical literature. London: Arts Council England, 2004.
- 3. Nilsson U. The anxiety- and pain-reducing effects of music interventions: a systematic review. AORN J 2008; 87: 780-807.
- 4. Padmanabhan R, Hildreth AJ, Laws D. A prospective, randomised, controlled study examining binaural beat audio and pre-operative anxiety in patients undergoing general anaesthesia for day case surgery. Anaesthesia 2005; 60: 874-877.
- 5. Oster G. Auditory beats in the brain. Scientific American 1978; 229: 94-102.
- 6. Le Scouarnec RP, Poirier RM, Owens JE, et al. Use of binaural beat tapes for treatment of anxiety: a pilot study of tape preference and outcomes. Altern Ther Health Med 2001; 7: 58-63.
- 7. Holm L, Fitzmaurice L. Emergency department waiting room stress: can music or aromatherapy improve anxiety scores? Pediatr Emerg Care 2008; 24: 836-838.
- 8. Menegazzi JJ, Paris PM, Kersteen CH, et al. A randomized, controlled trial of the use of music during laceration repair. Ann Emerg Med 1991; 20: 348-350.
- 9. Tanabe P, Thomas R, Paice J, et al. The effect of standard care, ibuprofen, and music on pain relief and patient satisfaction in adults with musculoskeletal trauma. J Emerg Nurs 2001; 27: 124-131.
- 10. Short A, Ahern N. Evaluation of a systematic development process: relaxing musing for the emergency department. Aust J Music Ther 2009; 20: 3-26.
- 11. Short A, Ahern N, Holdgate A, et al. Using music to reduce noise stress for patients in the emergency department: a pilot study. Music Med 2010; 2: 201-207.
- 12. Macarow K, Brown D, Jelinek G. Art does matter: designing sound compositions for emergency department patients [presentation]. Fifth International Conference on the Arts in Society; 22–25 July 2010; Sydney, Australia. Urbana-Champaign, Ill: Common Ground Publishing.
- 13. Australasian College for Emergency Medicine. Policies and guidelines. P06: Australasian Triage Scale. Melbourne: ACEM, 2000. http://www.acem.org.au/infocentre.aspx?docId=59 (accessed Nov 2010).
- 14. Spielberger CD, Gorsuch RL, Lushene R, et al. State–trait anxiety inventory. Menlo Park, Calif: Mind Garden Inc, 1970.
- 15. Bieling PJ, Antony MM, Swinson RP. The state-trait anxiety inventory, trait version: structure and content re-examined. Behav Res Ther 1998; 36: 777-788.
- 16. Wang SM, Kulkarni L, Dolev J, Kain ZN. Music and preoperative anxiety: a randomized, controlled study. Anesth Analg 2002; 94: 1489-1494.
- 17. Spielberger CD, Gorsuch RL, Lushene RE, et al. Manual for the State–Trait Anxiety Inventory. Palo Alto, Calif: Consulting Psychologists Press, 1983.
- 18. Jezova D, Makatsori A, Duncko R, et al. High trait anxiety in healthy subjects is associated with low neuroendocrine activity during psychosocial stress. Prog Neuropsychopharmacol Biol Psychiatry 2004; 28: 1331-1336.
- 19. Ruffinengo C, Versino E, Renga G. Effectiveness of an informative video on reducing anxiety levels in patients undergoing elective coronarography: an RCT. Eur J Cardiovasc Nurs 2009; 8: 57-61.
- 20. Tluczek A, Henriques JB, Brown RL. Support for the reliability and validity of a six-item state anxiety scale derived from the state-trait anxiety inventory. J Nurs Meas 2009; 17: 19-28.
Abstract
Objective: To determine whether emergency department (ED) patients’ self-rated levels of anxiety are affected by exposure to purpose-designed music or sound compositions with and without the audio frequencies of embedded binaural beat.
Design, setting and participants: Randomised controlled trial in an ED between 1 February 2010 and 14 April 2010 among a convenience sample of adult patients who were rated as category 3 on the Australasian Triage Scale.
Interventions: All interventions involved listening to soundtracks of 20 minutes’ duration that were purpose-designed by composers and sound-recording artists. Participants were allocated at random to one of five groups: headphones and iPod only, no soundtrack (control group); reconstructed ambient noise simulating an ED but free of clear verbalisations; electroacoustic musical composition; composed non-musical soundtracks derived from audio field recordings obtained from natural and constructed settings; sound composition of audio field recordings with embedded binaural beat. All soundtracks were presented on an iPod through headphones. Patients and researchers were blinded to allocation until interventions were administered. State–trait anxiety was self-assessed before the intervention and state anxiety was self-assessed again 20 minutes after the provision of the soundtrack.
Main outcome measure: Spielberger State–Trait Anxiety Inventory.
Results: Of 291 patients assessed for eligibility, 170 patients completed the pre-intervention anxiety self-assessment and 169 completed the post-intervention assessment. Significant decreases (all P < 0.001) in anxiety level were observed among patients exposed to the electroacoustic musical composition (pre-intervention mean, 39; post-intervention mean, 34), audio field recordings (42; 35) or audio field recordings with embedded bianaural beats (43; 37) when compared with those allocated to receive simulated ED ambient noise (40; 41) or headphones only (44; 44).
Conclusion: In moderately anxious ED patients, state anxiety was reduced by 10%–15% following exposure to purpose-designed sound interventions.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN 12608000444381.