





Volume 195 - Issue 11
Determining priority for joint replacement: comparing the views of orthopaedic surgeons and other professionals
Authors: Andrea J Curtis, Rory Wolfe, Colin O H Russell, Barry G Elliott, John A L Hart and John J McNeil
Med J Aust 2011; 195 (11): 699-702. || doi: 10.5694/mja10.11052
Published online: 12 December 2011
Published online: 12 December 2011
Abstract
Objective: To assess which patient characteristics influence the assessments of urgency for surgery by orthopaedic surgeons and non-orthopaedic professionals.
Design, setting and participants: Cross-sectional study of 80 patients requiring elective hip or knee replacement attending a public hospital orthopaedic outpatient clinic or orthopaedic surgeon’s private rooms. Patients were interviewed after being placed on the surgery waiting list. The interview asked about the severity of their joint disease and its effects on physical capability, psychological distress and social circumstances. Patient interviews were summarised and presented to assessors who ranked groups of eight patients in order of their perceived urgency for surgery. Eleven orthopaedic surgeon assessors completed 360 patient ratings and nine non-orthopaedic assessors from various professions, including physiotherapy, social work, research, management and engineering, completed 720 patient ratings.
Main outcome measures: Visual analogue scale rating of patient urgency for surgery; patient rankings for surgery; scores for individual domain contributions to urgency rating.
Results: A broad spread of perceived urgency was evident among the patients. For each group of eight patients, there was moderate agreement on overall urgency rankings between the two groups of assessors. Linear regression demonstrated that pain was the dominant determinant of urgency score for both assessor groups. Orthopaedic surgeons also took into account limitations to mobility and concurrent medical illness but gave less priority to psychological distress or social circumstances. For the non-orthopaedic assessors, limitations to mobility, social circumstances and psychological distress also contributed to urgency.
Conclusion: Both orthopaedic surgeons and non-orthopaedic professionals considered pain the most important factor in establishing urgency and priority for joint replacement. Only the non-orthopaedic professionals considered psychosocial factors important when determining priority for surgery. Broader community discussion about prioritisation for elective surgery is needed to facilitate agreement about which patients factors should be considered.
Total hip and knee arthroplasty are elective surgery procedures commonly undertaken at public hospitals in the United Kingdom, Canada and Australia, where they are associated with long waiting lists and waiting times. In 2008–2009, Australian national median waiting times were 95 days for hip replacement and 114 days for knee replacement.1 Australian elective surgery patients are classified into “urgent”, “semi-urgent” and “non-urgent” categories by their surgeons. There are no standardised criteria to guide classification and there is evidence of substantial inconsistency in the way surgeons assign urgency categories.2 Due to this informal approach to prioritisation, patients are not necessarily treated in order of urgency3 or severity of pain and disability.4 Age, sex, deprivation,5 employment status,6 educational status7 and marital status4 have all been linked with access to elective surgery. This is not an equitable, objective and transparent process for allocating surgery.
A more rational approach would determine priority for surgery with a specified set of clinical and non-clinical indicators to assess the impact of joint disease on the patient. Although Canadian and New Zealand tools have been developed to prioritise patients for joint replacement, these primarily reflect the views of surgeons and researchers.8-11 Little is known about how the general public perceives urgency for surgery, or which criteria should be considered in measuring urgency. Our study compares perceptions of urgency for surgery among a range of orthopaedic and non-orthopaedic assessors. We aimed to determine the relative importance of patient-related factors in the assessment of patients’ urgency for joint replacement.
Methods
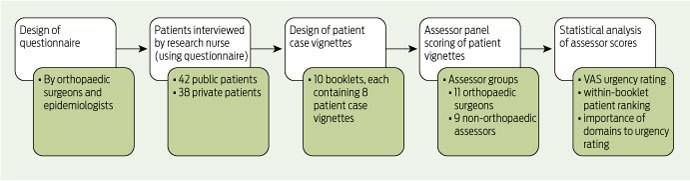
Our study method is outlined in Box 1, following the general method described elsewhere.12
The Alfred Hospital Human Research Ethics Committee approved this study. Patients gave informed consent to be included in the study.
Study questionnaire design
A questionnaire was developed by the study epidemiologists and orthopaedic surgeons to obtain information about the impact of joint disease on patients’ lives.
The questionnaire asked patients about the severity, frequency and duration of pain associated with their joint condition, and its impact on the patient’s life, including activities of daily living (ADL; defined as bathing, dressing, preparing meals and housework), social circumstances (including employment, carer responsibilities and use of support systems such as home help), psychological distress (including effect on emotions), and limitations to mobility (ability to walk and climb stairs, and use of walking aids). Other questions asked about comorbidities (eg, obesity, hypertension) and pain medications.
Patient recruitment
One-hundred and five patients with symptoms of joint disease considered by the treating orthopaedic surgeon to warrant joint replacement were recruited to the study during the appointment at which they were referred for surgery. Twenty-five patients did not participate further, as they had already undergone surgery, did not wish to take part, or were unsuitable for interview. Eighty patients joined the study. Forty-two patients were recruited from the outpatient clinic of a Victorian public hospital and 38 from participating surgeons’ private rooms.
Patient interview
Each patient was interviewed by a nurse using the study questionnaire. Interviews took place after the recruitment visit at a time convenient to the patient.
Domains and patient vignettes
The answers from each patient’s questionnaire were transcribed in the patient’s own words into a vignette. Each vignette contained seven domains corresponding to the questions in the study questionnaire: pain, ADL, limitations to mobility, social circumstances, psychological distress, medical comorbidities, and medications. Sets of 10 booklets were produced. Each booklet contained eight randomly assigned vignettes, as this was considered the maximum that assessors could reliably rank.
Review of patient vignette booklets
Each vignette booklet was scored by members of two assessor groups recruited from among the associates of the investigators: the orthopaedic group (comprising 11 orthopaedic surgeons recruited from two public hospitals in Melbourne) and the non-orthopaedic group (comprising nine people from varied professions including medical practice [not orthopaedic surgeons], physiotherapy, social work, management and engineering). All orthopaedic surgeon assessors were men, and five of the non-orthopaedic assessors were women. All assessors were aged over 18 years. Each assessor was requested to:
rank the eight patients described in each booklet in order of their perceived urgency for surgery;
assess overall urgency for surgery using a 100 mm visual analogue scale (VAS), where 0 mm represented not urgent and 100 mm represented most urgent; and
assess the level of importance they gave to each domain when determining the urgency rating (scored from 1 to 10, where 1 was not important and 10 was very important).
Statistical analysis
VAS urgency ratings followed a roughly normal distribution and were summarised with means and standard deviations (SD). Intraclass correlation coefficients (ICCs) were used to summarise agreement between assessors on VAS urgency ratings, domain scores, and booklet-specific numerical rankings.
Eight Spearman rank correlation coefficients were calculated per assessor, one per booklet, to describe the association between VAS urgency ratings and the 1-to-8 rankings of the patients in that booklet.
For each assessor group, univariate linear regression models were fitted to VAS urgency ratings, with each individual domain score included as the covariate in turn. Multivariate linear regression models were then used to include all domain scores and ascertain which domains contributed independently to VAS urgency. A final multivariate model included interactions between domain score and assessor group, to test whether the different groups had different relationships between domain score and VAS urgency.
Analyses were conducted with Stata 11 statistical software (StataCorp, College Station, Tex, USA).
Results
Eighty patients were recruited to the study. Mean age was 65 years (SD, 12 years), and 54% were women. The major diagnosis was osteoarthritis (79%). Other diagnoses were loose hip prosthesis (5%), avascular necrosis (4%), rheumatoid arthritis (4%) and other miscellaneous conditions (8%). Fifty-five per cent of patients required hip replacement and 45% required knee replacement. Both insured (46%) and uninsured (public) (53%) patients were represented. Using the national clinical urgency category system for elective surgery,13 5% of patients were classified as category 1 (urgent), 91% as category 2 (semi-urgent) and 4% as category 3 (non-urgent).
Agreement among assessors
The ranking of different patients within booklets was done with moderate agreement among all assessors (mean of booklet-specific ICC, 0.46). Agreement was similar among orthopaedic surgeons and non-orthopaedic assessors (ICC, 0.49 and 0.46, respectively).
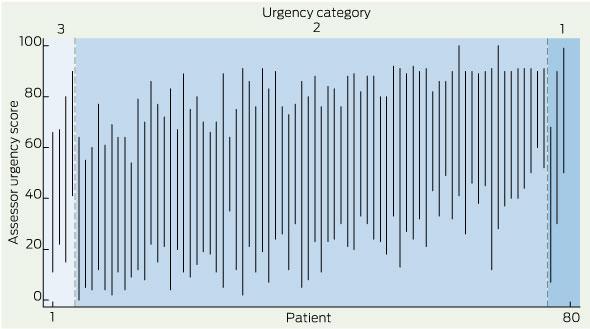
Distribution of urgency ratings
Assessor urgency ratings for each patient, presented in order of the urgency category assigned by their recruiting orthopaedic surgeon, are shown in Box 2. Within each urgency category, the patients are presented in order of mean VAS urgency rating, with each patient’s data presented as a line joining minimum to maximum VAS urgency rating. The results indicate considerable heterogeneity of perceived urgency among the patients in each category and substantial overlap between the perceived urgency of patients across the three categories.
Urgency ratings and rankings
There was a strong association between individual assessors’ VAS urgency ratings and their within-booklet 1-to-8 ranking of patients. The median Spearman correlation coefficient across all assessors and all booklets was − 0.9 (ranking decreased, ie, approached rank 1, as VAS urgency rating increased). Ninety-five per cent of these correlation coefficients were less than − 0.33.
VAS and domain scores
Mean VAS ratings and domain scores for each assessor group are summarised in Box 3. Each assessor group perceived that the pain domain was the most important contribution to their VAS urgency ratings. Both assessor groups also considered the limitations to the mobility domain to be important and the medications and medical comorbidities domains less important. In contrast to the orthopaedic assessors, the non-orthopaedic assessors considered the psychological distress and social circumstances domains to be important (Box 3).
Multivariate analysis (Box 4) demonstrated that the independent correlates of overall urgency varied between assessor groups. Pain and limitations to mobility correlated with urgency for both assessor groups, although the strength of this association varied by assessor group (P for interaction, 0.04 and 0.05 [for interactions of pain and limitations to mobility, respectively, with assessor group]).
Psychological distress, social circumstances, and ADL domains correlated significantly with urgency for the non-orthopaedic group but not among the orthopaedic surgeons (P for interaction, < 0.001, 0.05, and 0.2, respectively). There was an association between perceived urgency and medical comorbidities for orthopaedic surgeons but not for non-orthopaedic assessors (P for interaction, 0.001). The seven domains accounted for 53% and 37% of the variation in urgency ratings given by the non-orthopaedic and orthopaedic surgeon assessor groups, respectively.
Discussion
This study used vignettes derived from interviews with patients waiting for joint replacement surgery in a prioritisation exercise undertaken by orthopaedic surgeons and non-surgeons. The study allowed identification of the criteria that correlated best with the perceived patient urgency for surgery.
The assessors were able to discriminate between different levels of patient urgency using vignettes based on patient interviews. In general, assessors were able to put patients with similar results in order of priority, whether directly ranking patients against each other or using a VAS scale to assign a numerical score. For both assessor groups, pain was the domain most strongly and significantly associated with a patient’s urgency. For orthopaedic surgeons, the limitations to mobility and medical comorbidities domains were also significant predictors of patient urgency, but psychological distress, social circumstances and ADL were considered less important. This is consistent with other evidence indicating that surgeons place less priority on psychological characteristics when prioritising patients for joint replacement.14 We speculate that this is because surgeons find it difficult to assess non-clinical factors and use them to objectively compare the needs of different patients. For the non-orthopaedic assessors in this study, psychological distress, social circumstances and ADL made independent contributions to patient urgency, even after pain and limitations to mobility were taken into account.
A strength of this study was that the case vignettes used to assess urgency were derived from interviews with actual patients. This contrasts with the artificial vignettes often used in conjoint analysis methodology.
In addition to expert orthopaedic surgeons, the study assessors included non-orthopaedic assessors. Until recently, most surgery-related prioritisation studies have only included the views of surgeons and researchers. However, with involvement of the general public in priority setting being increasingly advocated, this is beginning to change. In a recent Spanish study, patients, patients’ relatives, the general public, medical consultants and allied health professionals were involved in identifying priority criteria.15 Also, the Victorian Multi-attribute Prioritisation Tool for joint replacement was developed through a concept-mapping process involving orthopaedic surgeons and patients.16 It is sometimes claimed that members of the public are biased and uninformed; however, all participants bring their own particular biases to priority setting exercises.17 While members of the public may not be experts in the ethical and clinical aspects of health care, they are likely to represent the values of wider society, and incorporation of their views may increase the acceptability of priority setting.18
Due to the time-consuming and complex nature of reviewing vignettes, only a small number of assessors participated in the study. Accordingly, the results obtained may not be representative of average public opinion. Additionally, the 80 recruited patients may not be representative of the broader orthopaedic patient community.
The seven domains included in the patient vignettes did not account for all variation in the assessors’ urgency ratings, reflecting the imperfect agreement among assessors and suggesting that other unknown factors may also contribute to urgency. Inclusion of some patients requiring revision surgery may have confounded overall urgency scoring.
To date, there is no gold standard list of the criteria that should contribute to a patient’s urgency and priority for surgery. Criteria such as pain, severity of symptoms and limitations to mobility are clearly important, but there is no consensus on other potentially relevant factors. This study demonstrated that pain and limitations to mobility are the principal patient-related criteria correlated with urgency, and that social circumstances, psychological distress and limitations to mobility are also considered important by non-orthopaedic assessors. We recommend that further studies of these criteria in relation to patient prioritisation should be undertaken.
In the future, there will be an increasing need to prioritise access to many forms of health care. Our study suggests that the community preference might be to take account of other factors, including measures of psychological distress and social dislocation.
2 Assessor urgency scores (n = 80), from non-urgent (category 3) to urgent (category 1)*
3 Visual analogue scale (VAS) urgency* and domain scores,† by assessor group
Competing interests
No relevant disclosures.
Acknowledgements
We thank the patients, research nurses, recruiting orthopaedic surgeons, and members of the assessor panel. The study was funded by the Victorian Department of Human Services.
References
- Australian Institute of Health and Welfare. Australian hospital statistics 2008–09. Canberra: AIHW, 2010. (AIHW Cat. No. HSE 84; Health Services Series No. 17.) 0_i1149983
- Russell C, Roberts M, Williamson TG, et al. Clinical categorisation for elective surgery in Victoria. ANZ J Surg 2003; 73: 839-842. 0_CHDBDDFJ
- Kelly KD, Voaklander DC, Johnston WC, Suarez-Almazor ME. Equity in waiting times for major joint arthroplasty. Can J Surg 2002; 45: 269-276. 0_i1149987
- Fitzpatrick R, Norquist JM, Reeves BC, et al. Equity and need when waiting for total hip replacement surgery. J Eval Clin Pract 2004; 10: 3-9. 0_i1149989
- Hacker J, Stanistreet D. Equity in waiting times for two surgical specialties: a case study at a hospital in the North West of England. J Public Health (Oxf) 2004; 26: 56-60. 0_i1149991
- Clover KA, Dobbins TA, Smyth TJ, et al. Factors associated with waiting time for surgery. Med J Aust 1998; 169: 464-468. 0_i1149993
- Siciliani L, Verzulli R. Waiting times and socioeconomic status among elderly Europeans: evidence from SHARE. Health Econ 2009; 18: 1295-1306. 0_i1149995
- Western Canada Waiting List Project. From chaos to order: making sense of waiting lists in Canada. Final report. Edmonton: WCWL, 2001. http://www.wcwl.org/media/pdf/library/final_reports.2.pdf (accessed Feb 2011).
- Noseworthy TW, McGurran JJ, Hadorn DC, Waiting for scheduled services in Canada: development of priority-setting scoring systems J Eval Clin Pract 2003; 9: 23-31. 0_pgfId-1149999
- Arnett G, Hadorn DC. Developing priority criteria for hip and knee replacement: results from the Western Canada Waiting List Project. Can J Surg 2003; 46: 290-296. 0_pgfId-1150000
- Hadorn DC, Holmes AC. The New Zealand priority criteria project. Part 1: Overview. BMJ 1997; 314: 131-134. 0_i1150001
- Curtis AJ, Wolfe R, Russell CO, et al. Prioritizing patients for prostatectomy: balancing clinical and psychosocial factors. ANZ J Surg 2007; 77: 112-117. 0_i1150003
- Street A, Duckett S. Are waiting lists inevitable? Health Policy 1996; 36: 1-15. 0_i1150005
- Glozier N, Groom G, Prince M. Patient psychological characteristics have minimal influence on surgical prioritization. Psychosom Med 2004; 66: 251-257. 0_i1150007
- Sampietro-Colom L, Espallargues M, Rodriguez E, et al. Wide social participation in prioritizing patients on waiting lists for joint replacement: a conjoint analysis. Med Decis Making 2008; 28: 554-566. 0_i1150009
- Osborne R, Haynes K, Jones C, et al. Orthopaedic Waiting List Project. Summary report. Melbourne: Victorian Department of Human Services, 2006. 0_i1150011
- Bruni RA, Laupacis A, Martin DK, et al. Public engagement in setting priorities in health care. CMAJ 2008; 179: 15-18. 0_i1150013
- Allepuz A, Espallargues M, Moharra M, et al. Prioritisation of patients on waiting lists for hip and knee arthroplasties and cataract surgery: instruments validation. BMC Health Serv Res 2008; 8: 76. 0_i1150017