





Volume 194 - Issue 5
Accidental ingestion of plastic from takeaway containers — food for thought
Authors: Marianne Guirgis, Robert Nguyen and Christopher Pokorny
Med J Aust 2011; 194 (5): 245-246. || doi: 10.5694/j.1326-5377.2011.tb02955.x
Published online: 7 March 2011
Published online: 7 March 2011
Foreign body oesophageal obstruction is a medical emergency. It may be accidental, particularly in children, or deliberate, for example with suicide attempts. We present two cases illustrating accidental oesophageal foreign body impaction occurring after consumption of food that had been heated in a plastic container in a microwave oven, then cut and eaten directly from the softened container. To date, we are not aware of any similar reports. In view of potential complications, care needs to be taken when food is eaten directly from plastic takeaway containers. (MJA 2011; 194: 245-246)
Clinical records
Patient 1
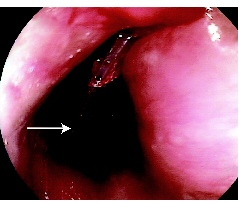
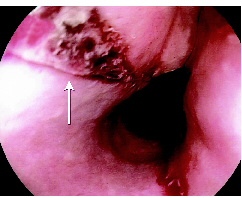
In April 2009, a 79-year-old woman was admitted to hospital with acute dysphagia. She had a history of hypertension, osteoporosis and hypercholesterolaemia. In the past she had also had a transient ischaemic attack. Her medications were felodipine, alendronate, atorvastatin and clopidogrel. Before presentation she had been eating quiche that had been heated in a plastic (polypropylene) container. At subsequent gastroscopy, a solid wedge-shaped piece of plastic 4 cm in length was found to be lodged in her upper oesophagus (Box 1). This was removed endoscopically with the aid of a stand
ard Roth Net retriever (US Endoscopy, Mentor, Ohio, USA) (a snare with a mesh basket) leaving a longitudinal mucosal tear (Box 2). There was no evidence of oesophageal perforation and she made a rapid and complete recovery, being discharged after 48 hours on pantoprazole in addition to her usual medications. At follow up after 2 weeks, she remained well and pantoprazole was ceased.
Patient 2
In October 2009, a previously well 45-year-old woman presented with sudden onset of odynophagia and dysphagia localised to the lower oesophagus after eating fish that had been stored and reheated in a clear polypropylene container. Initial ear, nose and throat assessment showed no evidence of fish bones in the tonsil area or oropharynx. A subsequent chest and neck computed tomography (CT) scan identified an opaque, linear foreign body within the subcarinal region of the oesophagus. There was no extraluminal gas or mediastinitis.
An urgent gastroscopy was arranged and revealed a superficial linear ulcer caused by a 3 cm × 2 cm plastic foreign body lodged in the mid-oesophagus. Attempted retrieval with grasping forceps failed and a Roth Net retrieval device was used to remove the piece of plastic through an overtube. A minor oesophageal mucosal tear was seen afterwards. The patient recovered uneventfully and was discharged after 24 hours.
Discussion
Foreign body impaction is an important cause of sudden-onset dysphagia and is a medical emergency. Foreign bodies can be classified either as food or true foreign bodies. In a recent retrospective series of 988 patients, the five most common foreign bodies resulting in impaction were food boluses (17.1%), coins (15.6%), fish bones (12.6%), dental prostheses (8.6%) and chicken bones (6%).1
The most common sites of impaction are the cricopharyngeus, aortic arch, left main branch bronchus and cardio-oesophageal junction, where physiological narrowing occurs. Objects greater than 2 cm have difficulty traversing the normal adult oesophagus.2 Risk factors for obstruction include young age, dentures, psychiatric disorders, neurological conditions such as motor neurone disease and strokes, developmental delay, impairment by alcohol and underlying oesophageal pathology.3 Oesophageal pathology includes inflammatory or fibrotic strictures, Schatzki rings, eosinophilic oesophagitis, malignancy and diverticula.4 Certain forms of obesity surgery, such as gastric banding, may also be complicated by dysphagia.
Clinical manifestations of oesophageal obstruction include chest pain, dysphagia, odynophagia, regurgitation and hypersalivation. Swelling, tenderness and crepitus may represent oropharyngeal or proximal oesophageal perforation. It is crucial to assess for airway compromise such as stridor, choking and coughing. This may result when the impaction occurs at the level of the upper oesophageal sphincter leading to tracheal compression. Complications of foreign body ingestion include obstruction, perforation, aspiration, tracheo-oesophageal fistula, aorto-oesophageal fistula, and abscess formation.5
Imaging such as x-ray or CT scan may demonstrate the location of the foreign body. Fish and chicken bones, glass, plastic, or food boluses may not always be seen on plain x-ray.
Most foreign bodies pass spontaneously, although up to 20% require intervention. Intravenous glucagon, which relaxes the oesophageal smooth muscle, may be administered before endoscopic therapy but is of limited value.6,7 Effervescent agents such as carbonated drinks are often given but evidence of their efficacy is limited and based on case series only.
Management is determined by the patient’s clinical condition and the anatomical location of the ingested material. Airway compromise or obstruction at the level of the cricopharyngeus may require consultation with an ear, nose and throat specialist. Otherwise, flexible endoscopy is the mainstay of foreign body removal.8 Success rates of 94% have recently been reported.1 In all cases, removal within 24 hours is recommended to avoid pressure-induced ischaemia and to minimise the risk of perforation.9 Urgent endoscopic removal is required when a sharp object is ingested or if evidence of high-grade obstruction is present. The foreign body may be removed using various instruments or by the push technique.3 The latter involves pushing the foreign body into the stomach with the endoscope but carries an increased risk of perforation.
Sharp objects represent a medical emergency due to the risk of perforation, which has been estimated to be as high as 35%.2 They are less common than other foreign bodies but more difficult to remove. Endoscopic removal with minimal mucosal injury can generally be achieved using a retrieval device such as a Roth Net, as in our cases, or polypectomy snares with use of an overtube.10 An algorithm for managing a suspected sharp oesophageal foreign body is outlined in Box 3.
The two cases we describe involved inadvertent ingestion of plastic as a result of cutting food in a heated, softened food container, resulting in a sharp foreign body oesophageal impaction and subsequent mucosal tear. To our knowledge, there have not been similar case reports in the literature. Given that takeaway food containers are widely used, these cases highlight the need for care to be taken when heating food in such containers and then consuming directly from them.
Competing interests
None identified.
References
- Li ZS, Sun ZX, Zou DW, et al. Endoscopic management of foreign bodies in the upper GIT-tract: experience with 1088 cases in China. Gastrointest Endosc 2006; 64: 485-492. 0_CIGJEJDC
- Duncan M, Wonk RK. Esophageal emergencies: things that will wake you from a sound sleep. Gastroenterol Clin North Am 2003; 32: 1035-1052. 0_CIGEBFEG
- Eisen GM, Baron TH, Dominitz JA, et al. Guideline for the management of ingested foreign bodies. Gastrointest Endosc 2002; 55: 802-806. 0_i1095906
- Cook I. Diagnostic evaluation of dysphagia. Nat Clin Pract Gastroenterol Hepatol 2008; 5: 393-403. 0_i1095908
- Ginsberg G. Management of ingested foreign objects and food bolus impactions. Gastrointest Endosc 1995; 41: 33-38. 0_i1095910
- Alaradi O, Bartholomew M, Barkin JS. Upper endoscopy and glucagons: a new technique in the management of acute esophageal food impaction. Am J Gastroenterol 2001; 96: 912-913. 0_i1095912
- Mehta D, Attia M, Quintana E, et al. Glucagon use for esophageal coin dislodgment in children: a prospective, double-blind, placebo controlled trial. Acad Emerg Med 2001; 8: 200-203. 0_i1095914
- Chaves DM, Ishioka S, Felix VN, et al. Removal of a foreign body from the upper gastrointestinal tract with a flexible endoscope: a prospective study. Endoscopy 2004; 36: 887-892. 0_i1095916
- Chaikhouni A, Kratz JM, Crawford FA. Foreign bodies of the esophagus. Am Surg 1985; 51: 173-179. 0_i1095919
- Jeen YT, Chun HJ, Song CW, et al. Endoscopic removal of sharp foreign bodies impacted in the esophagus. Endoscopy 2001; 33: 518-522. 0_i1095921