





Volume 194 - Issue 12
Lymphatic filariasis in Australia: an update on presentation, diagnosis and treatment
Authors: Cameron J Jeremiah, Craig A Aboltins and Peter A Stanley
Med J Aust 2011; 194 (12): 655-657. || doi: 10.5694/j.1326-5377.2011.tb03154.x
Published online: 20 June 2011
Published online: 20 June 2011
Clinical records
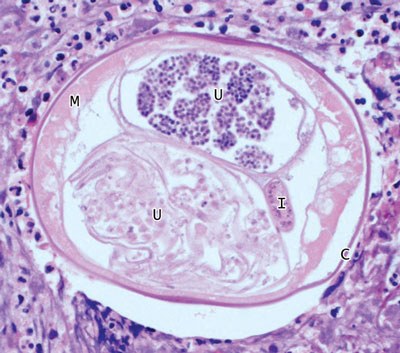
A 28-year-old man presented to the emergency department with a 2-day history of a right groin lump, scrotal discomfort and swelling. He was systemically well without urinary symptoms. The patient was born in Burma (Myanmar), and had migrated to Australia 6 years previously after living in Singapore for 2 years. On examination, there was an irreducible mass in the right inguinal canal, associated right scrotal swelling, and a normal testis. There was no peripheral blood eosinophilia. Ultrasonography showed a 1.1 cm heterogeneous right inguinal canal mass thought to be an incarcerated inguinal hernia. An inguinal incision was performed, and a mass attached to the spermatic cord was found and excised. Histopathology of the mass was consistent with filariasis (figure). Filarial serology (IgG enzyme immunoassay [EIA], Westmead Hospital, Sydney, NSW) was positive, but no microfilariae (filarial larvae) were seen on a blood film taken at 4 pm. The patient was treated with doxycycline 100 mg twice daily for 10 weeks and diethylcarbamazine 400 mg daily for 5 days, followed by 400 mg at 1 week and 1 month. Eighteen months later, the patient’s symptoms had not recurred.
A 29-year-old Indian man who had migrated to Australia 7 years previously was referred as an outpatient with 10 episodes of penile swelling over 18 months. The episodes began abruptly with fever, chills and myalgias, soon followed by diffuse penile swelling. The systemic features typically resolved over 24–48 hours, and the penile swelling over 3 days. There was some inguinal discomfort, but no urinary symptoms. On examination, small, tender, bilateral inguinal masses were palpable. Ten months before presentation, while visiting India, the patient had sought medical treatment for the same problem. A diagnosis of lymphatic filariasis (LF) was made, and treatment with diethylcarbamazine 300 mg daily for 3 months was started, but did not lead to improvement. Upon review in Australia, despite negative filarial IgG EIA and examination for circulating filarial antigen by immunochromatographic testing (Victorian Infectious Diseases Reference Laboratory, Melbourne, VIC), the clinical diagnosis of LF was thought to be correct. Twelve months after completing a 3-month course of doxycycline 100 mg twice daily the patient’s symptoms had not recurred.
A 57-year-old Samoan man was referred by his general practitioner to the emergency department with 2 weeks of right leg and left scrotal swelling. The patient had migrated to Australia 16 years previously, and had recently returned from a 1-month holiday in Samoa. He began to experience chills and sweats 2 months after returning, followed by progressive right calf and left scrotal swelling, erythema and heat over 2 weeks. He did not have pain or urinary symptoms. A moderate-sized left hydrocoele with induration of the overlying scrotal skin, and associated right inguinal lumps, were found on examination. Blood examination revealed mild eosinophilia (0.6 × 109/L, reference range [RR] 0–0.5 × 109/L), although a blood film for microfilariae was not obtained. Ultrasonography showed movement within a left-sided 6.9 × 5.7 × 7.3 cm hypoechoic scrotal mass and associated hydrocoele. The initial working diagnosis was combined cellulitis and epididymo-orchitis. Treatment with intravenous antibiotics was commenced, with little response. The hospital’s infectious diseases service reviewed the patient and advised that the presentation was more consistent with LF. Treatment with doxycycline 100 mg twice daily for 10 weeks was commenced. Filarial IgG EIA serology was negative. The patient’s symptoms resolved, including the hydrocoele, and 12 months later he had not experienced a recurrence.
Lymphatic filariasis (LF) is caused by the filarial nematodes Wuchereria bancrofti, Brugia malayi and Brugia timori, which are transmitted between definitive human hosts by multiple mosquito vectors and have varying geographical distributions. LF is common in tropical and subtropical regions — an estimated 120 million people in 81 countries are infected, a third of whom have overt clinical disease.1-2 About one-third of those infected reside in India, a third in Africa, and the remainder in the Americas, South-East Asia and the Pacific, including many of Australia’s neighbours and countries with which Australia shares strong migration links.1 It is difficult to estimate prevalence accurately, but according to antigenic studies, prevalence of LF infection in India (the country with the greatest disease burden) is 5.66%.2 Endemic LF transmission in Australia has not been reported for over 50 years.3All three of the patients described were originally from countries endemic for LF, and their cases highlight the need for clinicians to be aware of the likelihood of LF being imported into Australia. The patients presented with recurrent inguino-scrotal pathology, with or without associated systemic symptoms, emphasising the difficulties of diagnosing this infection.
LF manifestations may be acute or chronic. Acute adenolymphangitis, which is often recurrent, is characterised by fever, chills and lethargy, followed by focal and transient oedema, erythema and discomfort. Adult worms (macrofilariae) are usually concentrated in the inguinal and scrotal lymphatics, and thus lower-limb and inguinal symptoms are more common, although the upper limbs and breasts may be affected. Chronic LF infection is usually indicated by lower-limb lymphoedema, with or without ulceration. Other symptoms include hydrocoeles and chyluria.
In non-endemic regions, clinically apparent LF, manifested as adenolymphangitis, hydrocoeles or lymphoedema, is uncommon. Mosquitoes are inefficient vectors for LF — infection is generally restricted to migrants from endemic regions rather than travellers.4
Key clinical features that may assist in making a diagnosis of LF include:
history of residence in an endemic country for several years;
self-limiting nature of attacks, in contrast to bacterial cellulitis, incarcerated hernias or testicular torsion;
bilateral symptoms and signs, as described in Patient 3;
recurrent episodes, as in Patient 2;
palpable regional masses or lymphadenopathy.
Interestingly, many infected people remain asymptomatic. Risk factors for symptomatic disease include duration and intensity of exposure to vectors, adult worm burden, frequency of secondary infections and the host immune response.5
The diagnosis of symptomatic LF requires strong clinical suspicion. Careful ultrasound may identify the random movement of adult worms in dilated lymphatics, known as the “filarial dance sign” (FDS). This is particularly useful in a patient with scrotal symptoms and is considered the gold standard investigation for detecting viable adult worms;6 however, in Patient 3 this did not lead to the diagnosis.
A blood film and serological evaluation are alternative diagnostic options. In most endemic areas, circulating microfilariae (filarial larvae) exhibit nocturnal periodicity (coinciding with peak feeding of local mosquitos) and are best seen on blood films taken between 10 pm and 4 am. If nocturnal samples are not feasible, then provocation with diethylcarbamazine may enhance microfilarial detection 1–2 hours later. Pacific Island infections (except Papua New Guinea) are subperiodic, with maximal microfilaraemia in the late afternoon, and show unresponsiveness to provocation. Importantly, patients with the chronic manifestations of LF often have low levels of circulating microfilariae, resulting in lower blood-film sensitivity.7
Serological tests available in Australia include an in-house enzyme immunoassay (EIA) developed against the dog heartworm Dirofilaria immitis (Westmead Hospital, Sydney, NSW), and an EIA based on IgG4 antibodies to recombinant Bm14 filarial antigen (CELISA, Cellabs, Sydney, NSW).8 Estimates of D. immitis EIA sensitivity and specificity vary and have been limited by an absence of accurate comparators and cross-reactivity. The newer Bm14 test has shown promising sensitivity and specificity. Neither test can differentiate filarial species, or active infection from past infection.
Two tests that may be performed throughout the day are available for filarial antigen detection, which is a measure of adult worm burden (BinaxNOW Filariasis ICT [immunochromatographic test], Alere, Brisbane, QLD; and Og4C3 EIA, TropBio, Townsville, QLD).7 Both tests have limited sensitivity for diagnosing chronic disease manifestations — compared with ultrasound for live adult worms, ICT has 67% sensitivity. Neither test detects antigen from B. malayi or B. timori.6,7,9 BRUGIArapid ICT (Malaysian Biodiagnostics Research, Selangor Bangi, Malaysia) detects antibodies to B. malayi and B. timori only, but must be imported from Malaysia.
Biopsy may allow identification of adult worms, but, given the availability of less invasive tests, it is reserved for difficult diagnoses.
In non-endemic areas, the objective of LF treatment is symptom improvement rather than transmission reduction. Traditional LF treatments target microfilariae and have limited activity against macrofilariae. Macrofilariae and the host immune response are responsible for many disease manifestations, but recent evidence has implicated the symbiotic, intracellular bacteria Wolbachia in pathogenesis.5,10,11 Filarial nematodes depend on Wolbachia for normal development and fertility.10 Doxycycline has been shown to clear filaria of Wolbachia symbionts, leading to microfilarial and macrofilarial death, and thus provides an attractive treatment option.11-13
Multiple clinical trials have demonstrated doxycycline’s efficacy in reducing adult worm viability (as measured by scrotal ultrasound), circulating antigenaemia (a marker of adult worm burden) and microfilaraemia.11-13 The degree of reduction of adult worm viability with doxycycline (75%–92%) appears to be far greater than that with any of the commonly used antifilarial agents. Further, doxycycline has significant effects on disease progression, bringing about improvement in lymphatic function, hydrocoele size, lymphoedema, circulating levels of lymphangiogenic factors and rates of lymphangitis.11 The extent to which doxycycline’s effects are mediated through activity against secondary bacterial pathogens has not been evaluated.
The optimal dose and duration for doxycycline therapy is unclear, but studies using 200 mg daily for at least 6 weeks have shown the best results.11,13 Whether doxycycline should be used in conjunction with ivermectin, albendazole or diethylcarbamazine remains unknown. These additional drugs increase adverse events; however, few trials have compared combination regimens to doxycycline alone.12 Overall, the evidence suggests that in non-endemic settings doxycycline is the treatment of choice for symptomatic LF. All patients in this series demonstrated a good clinical response to doxycycline.
Lessons from practice
In non-endemic countries such as Australia, where lymphatic filariasis (LF) is uncommon and can masquerade as other illnesses, the diagnosis may be delayed or missed. A high degree of clinical suspicion should be maintained.
Manifestations of LF include acute adenolymphangitis characterised by acute episodic inguino-scrotal or lower-limb swelling and discomfort, often associated with systemic symptoms and chronic lymphatic dysfunction. Diagnosis is largely based on clinical features, owing to the limitations of diagnostic investigations.
There is growing evidence in support of doxycycline as an effective, well tolerated, affordable disease-modifying treatment that is active against Wolbachia, an essential filarial endosymbiont.
Competing interests
None identified.
References
- Lymphatic filariasis: epidemiology and risk factors (updated 24 Apr 2008). Atlanta: Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/dpd/parasites/lymphaticfilariasis/epidemiology_lymphatic_filar.htm (accessed Mar 2010).
- Michael E, Bundy DA, Grenfell BT. Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitology 1996; 112: 409-428. 0_i1095952
- Boreham PFL, Marks NM. Human filariasis in Australia: introduction, investigation and elimination. Proc R Soc Qld 1986; 97: 23-52. 0_i1095954
- Hairston NG, de Meillon B. On the inefficiency of transmission of Wuchereria bancrofti from mosquito to the human host. Bull World Health Organ 1968; 38: 935-941. 0_i1095956
- Taylor MJ, Hoerauf A, Bockarie M. Lymphatic filariasis and onchocerciasis. Lancet 2010; 376: 1175-1185. Epub 2010 Aug 23. 0_i1095958
- Amaral F, Dreyer G, Figueredo-Silva J, et al. Live adult worms detected by ultrasonography in human Bancroftian filariasis. Am J Trop Med Hyg 1994; 50: 753-757. 0_i1095960
- Chanteau S, Moulia-Pelat JP, Glaziou P, et al. Og4C3 circulating antigen: a marker of infection and adult worm burden in Wuchereria bancrofti filariasis. J Infect Dis 1994; 170: 247-250. 0_i1095962
- Lammie PJ, Weil G, Noordin R, et al. Recombinant antigen-based antibody assays for the diagnosis and surveillance of lymphatic filariasis — a multicenter trial. Filaria J 2004; 3: 9. 0_i1095964
- Dreyer G, Lins R, Noroes J, et al. Sensitivity of the immunochromatographic card test relative to detection of adult Wuchereria bancrofti worms by ultrasound. Am J Trop Med Hyg 2008; 78: 28-34. 0_i1095966
- Taylor MJ, Bandi C, Hoerauf A. Wolbachia bacterial endosymbionts of filarial nematodes. Adv Parasitol 2005; 60: 245-284. 0_i1095968
- Debrah AY, Mand S, Specht S, et al. Doxycycline reduces plasma VEGF-C/sVEGFR-3 and improves pathology in lymphatic filariasis. PLoS Pathog 2006; 2: e92. 0_i1095970
- Supali T, Djuardi Y, Pfarr KM, et al. Doxycycline treatment of Brugia malayi-infected persons reduces microfilaremia and adverse reactions after diethylcarbamazine and albendazole treatment. Clin Infect Dis 2008; 46: 1385-1393. 0_i1095972
- Taylor MJ, Makunde WH, McGarry HF, et al. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. Lancet 2005; 365: 2116-2121. 0_i1095976
Provenance: Not commissioned; externally peer reviewed.