





Volume 193 - Issue 7
Catching a chameleon: IgG4-related systemic disease
Authors: Eu Jin Lim, Prithi S Bhathal, Peter P Tagkalidis and Antony G Speer
Med J Aust 2010; 193 (7): 418-420. || doi: 10.5694/j.1326-5377.2010.tb03974.x
Published online: 4 October 2010
Published online: 4 October 2010
IgG4-related systemic disease (IRSD) is a recently described entity with protean manifestations. We describe a patient who developed inflammation and fibrosis in multiple organs over 20 years, sequentially involving his pancreas, bile ducts, gallbladder, submandibular and lacrimal glands, and kidneys. He had an elevated serum IgG4 level. Retrospective analysis of biopsies showed strongly positive tissue immunostaining for IgG4, confirming the diagnosis of IRSD. This case illustrates the natural history of partially treated IRSD and its varied clinical presentations. Early diagnosis and treatment is important, as the condition is highly steroid-responsive.
Clinical record
A 55-year-old man who abstained from drinking alcohol and was not taking any medications initially presented to a hepatobiliary surgeon in 1989 for recurrent abdominal pain and jaundice. On examination, he was icteric, with mild epigastric tenderness, but was afebrile and had no other signs of chronic liver disease. His serum amylase level was mildly elevated, and results of liver function tests (LFTs) showed abnormal levels of albumin (29 g/L; reference range [RR], 36–48 g/L), alkaline phosphatase (284 U/L; RR, 32–91 U/L), γ-glutamyltransferase (98 U/L; RR, < 38 U/L), alanine transaminase (50 U/L; RR, < 34 U/L) and bilirubin (102 μmol/L; RR, < 18 μmol/L).
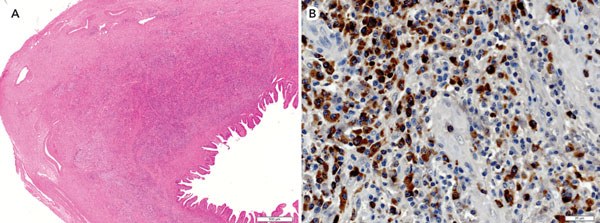
An abdominal computed tomography (CT) scan showed a 6 cm mass in the head of the pancreas consistent with a carcinoma. At laparotomy, his pancreas was noted to be hard and thickened. An intraoperative cholangiogram revealed multiple bile duct strictures. A cholecystectomy and side-to-side choledochojejunostomy were performed. Biopsy of the pancreatic mass showed mature fibrocollagenous connective tissue with scattered plasma cells, but no evidence of malignancy. The liver biopsy showed features consistent with large bile duct obstruction. Histological examination of the cystic duct and gallbladder showed diffuse lymphoplasmacytic infiltration, with intervening areas of dense fibrosis, causing marked wall thickening (Box 1, A). No gallstones were found. Rectal biopsies performed later were normal, excluding ulcerative colitis. A diagnosis of chronic idiopathic pancreatitis and primary sclerosing cholangitis (PSC) was made. His symptoms waxed and waned with no specific treatment.
In 1993, the patient presented to a rheumatologist with dry mouth, without dry eyes, and was noted to have bilateral submandibular gland swelling and exophthalmos from bilateral lacrimal gland enlargement. He was otherwise well, with no history of rash, myalgia or arthritis. His erythrocyte sedimentation rate (ESR) was 29 mm/h (RR, 7–18 mm/h). No antinuclear antibodies or antineutrophil cytoplasmic antibodies were detected. A percutaneous Trucut biopsy of the submandibular gland showed a dense lymphoplasmacytic infiltrate and prominent fibrosis. Lymphoepithelial lesions were present without morphological features of lymphoma. A diagnosis of seronegative Sjögren’s syndrome was made, and the patient was given a trial of steroid treatment, starting with 30 mg of prednisolone daily. His exophthalmos and submandibular gland swelling resolved over 3 months, and no abnormality was seen on a repeat orbital CT scan. Incidentally, his abdominal pain resolved and his LFT results returned to normal. The prednisolone dose was reduced over 12 months to 5 mg/day.
In 2002, with a serum creatinine level of 180 μmol/L (RR, 64–104 μmol/L) and a urea level of 13.5 mmol/L (RR, 2.5–8.3 mmol/L), the patient was referred to a nephrologist. Antinuclear antibodies were detected at a high titre of 1 : 640, and his ESR was 45 mm/h. The patient had eosinophilia (0.9 × 109 cells/L; RR, 0–0.5 × 109 cells/L), with an otherwise normal full blood count. His serum IgE level was normal. His spot urine protein–creatinine ratio was 89 mg/mmol (RR, 15–35 mg/mmol), consistent with proteinuria. A renal biopsy showed interstitial oedema; marked fibrosis with a dense infiltrate of lymphocytes, plasma cells and eosinophils; and moderate tubular atrophy, indicating severe active chronic tubulointerstitial nephritis. The patient’s prednisolone dose was increased to 60 mg/day, resulting in a dramatic improvement in renal function and normalisation of the spot urine protein–creatinine ratio. His steroid dose was tapered over the next few years.
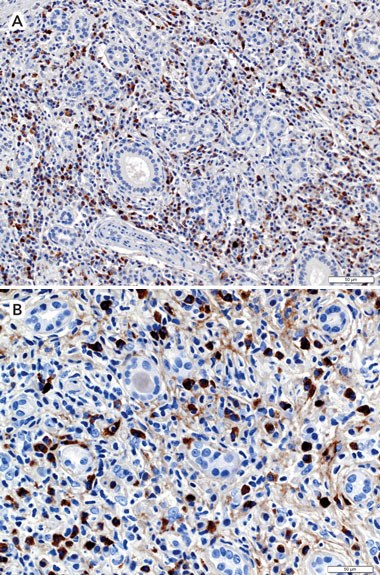
In 2009, the patient was referred to our gastroenterology clinic. His history of a benign pancreatic mass with biliary strictures was typical for autoimmune pancreatitis, and a diagnosis of IgG4-related systemic disease (IRSD) was considered. His IgG level was elevated (23.3 g/L; RR, 5.0–16.0 g/L), but IgM and IgA levels were in the normal range. In particular, the IgG4 subclass was markedly elevated, at 12.2 g/L (RR, 0.04–0.86 g/L). Levels of all other IgG subclasses fell within the normal range. The patient’s earlier biopsy samples were retrieved and immunostained for IgG4 using a recently commercially available monoclonal antibody (Zymed Laboratories Inc, San Francisco, Calif, USA). Strongly positive immunostaining for IgG4 was seen in the gallbladder, cystic duct (Box 1, B), submandibular gland (Box 2, A), lacrimal gland and kidney (Box 2, B) biopsies compared with control staining for total IgG. The proportions of IgG4-positive plasma cells (relative to total IgG-positive plasma cells) in the cystic duct, submandibular gland and kidney were 89%, 45% and 66%, respectively. These high proportions of IgG4-positive plasma cells (> 40%) confirmed the diagnosis of IRSD.1
Discussion
Recurrent abdominal pain and elevated serum amylase levels had first developed in our patient 20 years previously. He was given the diagnosis of chronic idiopathic pancreatitis, as the concept of autoimmune pancreatitis was not reported until 5 years later.2 Autoimmune pancreatitis may present with recurrent abdominal pain and jaundice, and a pancreatic mass indicative of carcinoma is commonly seen on imaging. The diagnosis of autoimmune pancreatitis can be suggested by an elevated serum IgG4 level3 and confirmed by biopsy showing a dense lymphoplasmacytic infiltrate with numerous IgG4-positive plasma cells.1,4 Patients usually respond well to treatment with steroids.
Our patient’s cholestatic LFT results and biliary strictures were ascribed to PSC. However, gallbladder and cystic duct histology revealed a lymphoplasmacytic infiltrate rich in IgG4-positive cells with associated obliterative phlebitis, typical of lymphoplasmacytic sclerosing cholangitis.5 An elevated serum IgG4 level is seen in 75% of patients with this condition, and steroid therapy usually normalises LFT results and biliary strictures, a feature not seen in PSC.6 Our patient also had chronic sclerosing cholecystitis.
Although our patient’s chronic sclerosing sialadenitis and dacryoadenitis were attributed to Sjögren’s syndrome, his exocrine gland histology was more consistent with Mikulicz’s disease, which differs from Sjögren’s syndrome both clinically and histopathologically. Mikulicz’s disease is associated with prominent infiltration of IgG4-positive plasma cells into lacrimal and salivary glands, as well as a favourable response to corticosteroid treatment.7 Also, lacrimal gland tear production is preserved in Mikulicz’s disease but not in Sjögren’s syndrome,8 as was noted in our patient.
Tubulointerstitial nephritis is the most common form of IgG4-related renal disease. Characteristically, the renal tubulointerstitium is infiltrated by large numbers of IgG4-positive plasma cells and eosinophils, resulting in cortical fibrosis and tubular atrophy.9 This condition is frequently associated with eosinophilia and proteinuria, and responds well to high-dose corticosteroid treatment, leading to improved renal function and reduced proteinuria. IgG4-associated membranoproliferative glomerulonephritis has also been reported.
IRSD can manifest in varied clinical presentations (Box 3), unified by characteristic histological findings of diffuse IgG4-positive plasma cell infiltration of multiple organs, resulting in obliterative phlebitis and tissue fibrosis.10 Our case illustrates the potentially chronic natural history of partially treated IRSD leading to presentations to different medical specialists over 20 years, emphasising the importance of diagnosing IRSD in order to institute treatment with steroids.
Competing interests
1 Biopsy samples of the patient’s cystic duct
2 Biopsy samples of the patient’s submandibular gland and kidney
 |
|
Biopsy samples showing numerous IgG4-immunopositive plasma cells (monoclonal antibody stain). A: Submandibular gland (original magnification, × 200). B: Kidney (original magnification, × 400). |
3 Manifestations of IgG4-related systemic disease
Autoimmune pancreatitis*
Lymphoplasmacytic sclerosing cholangitis*
Lymphoplasmacytic sclerosing cholecystitis*
Chronic sclerosing sialadenitis*
Chronic sclerosing dacryoadenitis*
Chronic tubulointerstitial nephritis*
Membranoproliferative glomerulonephritis
Autoimmune hepatitis
Riedel’s thyroiditis
Interstitial pneumonia
Pseudotumours of the lung
Lymphoplasmacytic aortitis
Hypophysitis resulting in hypopituitarism or diabetes insipidus
References
- Cheuk W, Yuen HKL, Chu SYY, et al. Lymphadenopathy of IgG4-related sclerosing disease. Am J Surg Pathol 2008; 32: 671-681. 0_i1095464
- Yoshida K, Toki F, Takeuchi T, et al. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci 1995; 40: 1561-1568. 0_i1095466
- Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 2001; 344: 732-738. 0_i1095468
- Tabata M, Kitayama J, Kanemoto H, et al. Autoimmune pancreatitis presenting as a mass in the head of the pancreas: a diagnosis to differentiate from cancer. Am Surg 2003; 69: 363-366. 0_i1095470
- Nakanuma Y, Zen Y. Pathology and immunopathology of immunoglobulin G4-related sclerosing cholangitis: the latest addition to the sclerosing cholangitis family. Hepatol Res 2007; 37 Suppl 3: S478-S486. 0_i1095472
- Ghazale A, Chari ST, Zhang L, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology 2008; 134: 706-715. 0_i1095474
- Tsubota K, Fujita H, Tsuzaka K, Takeuchi T. Mikulicz’s disease and Sjögren’s syndrome. Invest Ophthalmol Vis Sci 2000; 41: 1666-1673. 0_i1095476
- Mehta M, Jakobiec F, Fay A. Idiopathic fibroinflammatory disease of the face, eyelids, and periorbital membrane with immunoglobulin G4-positive plasma cells. Arch Pathol Lab Med 2009; 133: 1251-1255. 0_i1095478
- Watson SJ, Jenkins DA, Bellamy CO. Nephropathy in IgG4-related systemic disease. Am J Surg Pathol 2006; 30: 1472-1477. 0_i1095480
- Khosroshahi A, Stone JR, Pratt DS, et al. Painless jaundice with serial multi-organ dysfunction. Lancet 2009; 373: 1494. 0_i1095483