





Volume 190 - Issue 11 Supplement
Pushing the envelope: clinical handover from the aged-care home to the emergency department
Authors: Mary K Belfrage, Clare Chiminello, Diana Cooper and Sally Douglas
Med J Aust 2009; 190 (11 Suppl): S117. || doi: 10.5694/j.1326-5377.2009.tb02616.x
Published online: 1 June 2009
Published online: 1 June 2009
Abstract
Objective: To evaluate the use and usefulness of an aged-care home (ACH) transfer-to-hospital envelope (the Envelope) as a tool to support safe clinical handover when an ACH resident is transferred to an emergency department (ED).
Design, setting and participants: Participants in the study were 26 ACHs (1545 beds), the EDs of six major metropolitan public teaching hospitals in Melbourne, and ambulance officers involved in transferring residents from ACHs to hospitals. Transfer data were collected over an 18-week period (January–May 2008). Evaluation methods included written surveys and semi-structured face-to-face interviews (interviewees were 19 ACH staff, 30 ED staff, and 7 ambulance officers familiar with the Envelope).
Main outcome measures: Use, usefulness and ease of use of the Envelope; impact of using the Envelope on clinical handover; awareness of the need for clinical handover; sustainability of the project.
Results: The Envelope was used for the large majority of ACH residents transferred to hospital (ACH data: 317/355 [89%]; ED data: 85/101 [84%]); 163/165 ACH staff (99%) thought the Envelope was useful, and 148/165 (90%) said it was easy to use; 128/165 ACH staff (78%) and all interviewees believed that using the Envelope improved clinical handover; and 152/165 ACH staff (92%) indicated they would continue to use the Envelope. All interviewees thought that using the Envelope had raised awareness of the need for clinical handover.
Conclusion: The Envelope is useful and easy to use. It is used in the large majority of transfers of ACH residents to EDs and is highly valued by ACH staff, ambulance officers and ED staff. Our results suggest that use of the Envelope makes clinical handover safer for patients.
The residential aged-care sector is often overlooked when patient safety issues are considered. This is exemplified by the paucity of literature about clinical handover between aged-care homes (ACHs) and hospitals.1-3 Residents of ACHs are elderly, usually frail, and almost always have complex care needs. They often need to go to hospital — usually at short notice to an emergency department (ED), but also for planned admissions or to attend outpatient appointments. The transfer of ACH residents between ACHs and the acute sector involves a number of clinical handovers (between ACH staff, and between ambulance officers [AOs] and hospital staff) and a number of communication modalities (face-to-face, via telephone, by documents and — occasionally, but probably increasingly — electronically). The multiplicity of factors generates a high risk of communication failure and unsafe clinical handover, which can have a direct impact on the continuity of care and health outcomes for this population.3,4
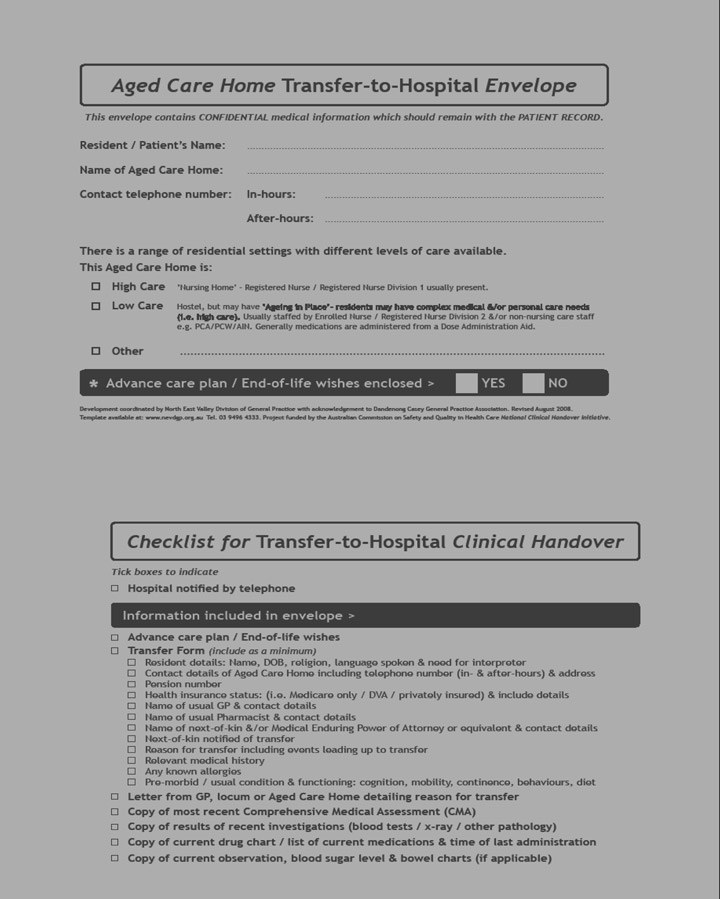
As part of the Aged Care General Practitioner Panels Initiative (ACGPPI),5 we developed an “Aged care home transfer-to-hospital envelope” (the Envelope) (Box 1) in response to frequent anecdotal reports from ACH and ED staff about the poor quality of transfer and discharge information (clinical handover) accompanying residents both to and from hospital. We identified several reasons why clinical handover was frequently so poor between these health care settings.6 Firstly, there is limited understanding of the range of constraints affecting the provision of care in each setting. Secondly, there are workforce issues that have a direct impact on both reasons for transfer to hospital and the provision of clinical handover. These include limited access to timely and regular medical care, the skills mix of the residential aged-care workforce, and frequent turnover of staff in both ACH and ED settings (recruitment and retention issues as well as shift-to-shift and staff rotation issues). Thirdly, ACH staff frequently reported that clinical and other handover information they had provided did not reach the ED but disappeared into a so-called “black hole”. In addition, we commonly had the impression, from discussions with both ACH and ED staff, that clinical handover was not really recognised as necessary. There was a sense that, once the resident/patient was “sent off”, the responsibility for care was discharged and that “they” (ED or ACH staff, respectively) would take over effective care (without awareness of the need to provide handover information).
Clinical handover is required both when a resident is transferred to hospital and when he or she is discharged to the ACH. The Envelope was designed specifically to support clinical handover when a resident is transferred to hospital. An envelope is a familiar communication tool. As well as its traditional function of containing documents for transfer from one place to another, the back of the Envelope features a checklist of key clinical and other handover information needed when a resident is transferred from an ACH to an ED.
We set out to evaluate the use and usefulness of the Envelope as a tool to support safe clinical handover from the ACH to the ED, and to raise awareness of the need for clinical handover between these settings. Throughout the trial, we sought feedback on the layout, design and content of the Envelope and on factors that would support ongoing and national use of the Envelope.
In the trial, our focus was on the ED, as the most common destination for transfer. Clinical handover at discharge from hospital to the ACH is a separate process requiring further study.
Methods
Participants
Participants in the trial were 26 ACHs (1545 beds) and the EDs of six major public teaching hospitals across inner city, inner east, north east, northern and western metropolitan Melbourne, as well as ambulance services involved in the transfer of residents from the 26 ACHs to hospital. The sample of ACHs recruited represented different provider models; cultural, socioeconomic and geographical diversity; varying size; and different levels of care provision.
Management structure
The North East Valley Division of General Practice was the lead agency in the trial, which was conducted by a consortium of seven Divisions of General Practice. The management structure for the trial consisted of a project team, a management group and a reference group (Box 2).
Approach
We used a highly collaborative and consultative approach. Based on regular feedback, refinements were made to trial processes and tools, including the content and format of the Envelope.
In addition, the principles that governed the information “fields” included on the Envelope were (i) maintaining privacy of the resident (no clinical information is recorded on the Envelope); (ii) evidence to support inclusion or exclusion of content; (iii) succinct and simple design and content; (iv) appropriateness for use nationally; and (v) keeping costs to a minimum.
Phases of the trial
The trial was conducted from September 2007 to October 2008 in three phases:
Engagement and recruitment of stakeholders and development of trial tools (September to January). Effective working relationships had been established between Divisions of General Practice and ACHs through the ACGPPI. Divisions of General Practice had longstanding relationships with hospitals, which were further enhanced by work undertaken as part of the ACGPPI. This enabled recruitment to the trial and the keen participation of ACHs and EDs. Specific investment was made to engage with and recruit ambulance services, as AOs are key stakeholders in this particular clinical handover scenario.
Data collection by ACHs and EDs on use of the Envelope each time a resident was transferred to hospital during the period January–May 2008 (18 weeks) was overseen by a designated person in each ACH and each ED. ACHs submitted data forms weekly by fax. Project officers personally collected ED data forms each week. This built in the regular opportunity to meet with ED staff at each hospital to discuss strategies to improve data collection. In addition, we had access to routinely collected transfer data supplied by the Metropolitan Ambulance Service (now Ambulance Victoria).
Evaluation and reporting (May to October). Evaluation methods used were:
Written surveys completed by ACH staff (165);
Semi-structured, face-to-face targeted interviews with ACH staff (19);
Semi-structured, face-to-face targeted interviews with ED staff (10 staff in three EDs);
Group interviews with ED staff (12 staff in two EDs);
Discussion group with ED staff, each completing an interview proforma (8 staff in one ED);
Semi-structured, face-to-face opportunistic interviews with AOs (11 in total, of which seven were familiar with the Envelope); and
Feedback and consultation with the management group and reference group.
The final report was lodged with the Australian Commission on Safety and Quality in Health Care in October 2008.6
Results
Use of the Envelope
Recorded ACH data indicated that a total of 417 residents were transferred from trial ACHs to hospitals during the trial period. Of these, 355/417 (85%) were transferred to EDs participating in the trial. The Envelope was used for 317/355 of transfers (89%). Recorded ED data indicated fewer transfers — 101 in total from trial ACHs — with 85/101 (84%) arriving in the ED with the Envelope. Ambulance data recorded a total of 577 transfers from trial ACHs to hospitals, of which 497/577 (86%) were transferred to trial EDs. Use of the Envelope was not recorded by Ambulance Victoria.
Usefulness of the Envelope
Almost all the ACH staff surveyed (163/165 [99%]) indicated that the Envelope was useful (Box 3), and 148/165 (90%) thought it was easy to use.
All 30 ED staff interviewed reported that the information about the ACH level of care was useful for background knowledge of the residential aged-care sector and for discharge planning.
All seven AO interviewees who were familiar with the Envelope reported that handover information was more organised when the Envelope was used.
Impact on clinical handover
About three-quarters of ACH staff (128/165 [78%]) believed that using the Envelope always or usually improved clinical handover from the ACH to the ED; 138/165 (84%) indicated that using the Envelope always or usually improved clinical handover from the ACH to AOs.
All interviewees (19 ACH staff, seven AOs familiar with the Envelope, and 30 ED staff) believed that using the Envelope had improved clinical handover.
Sustainability of Envelope use
Most ACH staff (152/165 [92%]) indicated that they would continue to use the Envelope, and 151/165 (91%) said they would recommend the Envelope be used if they moved to an ACH that did not use it.
All 19 ACH interviewees reported that the Envelope was embedded in their transfer process and that they would continue to use it beyond the trial.
All 11 AOs and all 30 ED staff interviewed said they would support the use of the Envelope in all ACH resident transfers to hospital.
Discussion
Our results clearly show that the Envelope was used in the large majority of transfers of ACH residents to EDs. It was reported as easy to use, useful and highly valued by all parties involved in clinical handover from the ACH to the ED. There was a high level of support for its ongoing use.
The checklist of clinical and other handover information was particularly valued. It was developed and refined through a process of extensive consultation with all stakeholders, both before and during the trial, so we are confident that all key handover information is included.
An envelope is a low-cost, familiar, age-old communication tool and the instructions on the Envelope we designed and refined are simple and clear. The Envelope can function as a stand-alone tool, requiring minimal support and training for its implementation and use. The key challenges for ongoing and wider use of the Envelope are about supply and distribution (Box 4).
Our results suggest that using the Envelope improved clinical handover. This is supported by the consistent finding that ACH staff, AOs and ED staff believed that clinical handover was better when the Envelope was used. Given the established links between the quality of clinical handover, continuity of care and patient outcomes, it is likely that the Envelope is an effective means of improving the safety and quality of clinical handover and, therefore, of patient care.
We note the discrepancy in background data on the number of resident transfers to hospital recorded from each data source (ACHs, EDs and Ambulance Victoria). However, in our view, this does not affect the main outcomes of the trial.
Previously we had observed widely variable awareness of the need for clinical handover between ACHs and hospitals. This was the case among some staff in both ACH and ED settings and consequently informed one of the key objectives of the trial, which was to raise awareness of the need for clinical handover in this situation. The finding that all interviewees in the trial (ACH, ambulance and ED staff) believed that using the Envelope raised this awareness indicates that this objective was met.
Further work is needed in the area of provision of safe clinical handover in the reciprocal scenario — that is, when a patient is discharged from hospital to an ACH.
2 Management structure of the Envelope trial
Clinical advisor, project manager and two project officers
Aged-care program coordinators from each of the seven Divisions of General Practice and the two project officers
Representatives from aged-care homes; each emergency department participating in the trial; ambulance services; general practitioners; state and national peak bodies of Divisions of General Practice; the Medical Deputising Service; the Department of Human Services, Victoria (acute and aged-care divisions); and Carers Victoria (a consumer organisation)
4 Access to and supply of the Envelope
Free website access: A template will be available on the website of the Australian Commission on Safety and Quality in Health Care (http://www.safetyandquality.gov.au) and the North East Valley Division of General Practice (http://www.nevdgp.org.au)
Commercial printing and distribution: The Envelope is available for purchase from Compact Business Systems (http://www.compact.com.au)
Competing interests
None identified.
Acknowledgements
The Envelope was developed under the Aged Care GP Panels Initiative (2004–2008), funded by the Australian Department of Health and Ageing. The project was coordinated by the North East Valley Division of General Practice, with acknowledgement to Dandenong Casey General Practice Association for the original idea of a dedicated ACH-to-hospital transfer envelope. The Envelope trial was funded by the Australian Department of Health and Ageing through the Australian Commission on Safety and Quality in Health Care’s National Clinical Handover Initiative. We acknowledge the contribution of our partner Divisions of General Practice: Impetus, Melbourne East General Practice Network, Melbourne General Practice Network, Northern Division of General Practice, Pivot West and Westgate General Practice Network; staff of all ACHs, EDs and ambulance services involved in the trial; and members of the reference group, for invaluable input to the project and commitment to improving the care of older people in residential care. Thanks to Dr Andrew Dent, former Director of the ED at St Vincent’s Hospital, Melbourne, for the birth of the checklist.
References
- Crilly J, Chaboyer W, Wallis M. Continuity of care for acutely unwell older adults from nursing homes. Scand J Caring Sci 2006; 20: 122-134. 0_i1091951
- Hickman L, Newton P, Halcomb EJ, et al. Best practice interventions to improve the management of older people in acute care settings: a literature review. J Adv Nurs 2007; 60: 113-126. 0_pgfId-1095959
- Wong MC, Yee KC, Turner P. A structured evidence-based literature review regarding the effectiveness of improvement interventions in clinical handover. eHealth Services Research Group, University of Tasmania, for the Australian Commission on Safety and Quality in Health Care, 2008. http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/PriorityProgram-05 (accessed Feb 2009).
- Pothier D, Monteiro P, Mooktiar M, Shaw A. Pilot study to show the loss of important data in nursing handover. Br J Nurs 2005; 14: 1090-1093. 0_i1091956
- Australian Department of Health and Ageing. Aged Care General Practitioner Panels Initiative handbook. http://www.health.gov.au/internet/main/publishing.nsf/Content/aged-care-gp-toc (accessed Mar 2009).
- Belfrage M, Chiminello C, Cooper D, Douglas S. Final report: aged care home transfer-to-hospital envelope trial. Melbourne: North East Valley Division of General Practice, 2008. http://www.nevdgp.org.au/files/primarycaresupport/agedcareinitiative/Final%20Report%20% 20ACH%20Transfer-to-Hospital%20Envelope%20Trial%20October%202008.pdf (accessed Mar 2009).