





Volume 187 - Issue 7
Apparent spontaneous complete regression of a multifocal malignant mesothelioma of the pleura
Author: Roger K A Allen
Med J Aust 2007; 187 (7): 413-415. || doi: 10.5694/j.1326-5377.2007.tb01315.x
Published online: 1 October 2007
Published online: 1 October 2007
A 61-year-old woman diagnosed with multifocal, poorly differentiated epithelial mesothelioma in September 2002 went into sustained spontaneous remission within months. She was completely disease-free within 6 months, and remained so 5 years later. This case demonstrates that this tumour may, very rarely, regress spontaneously, with no recurrence for many years. A greater knowledge of the underlying immune mechanisms would aid future management of this and other tumours.
Clinical record
In early September 2002, a 61-year-old woman was referred to our centre from the emergency room of a local private hospital. She had presented with a 2-day history of intermittent, sudden onset, severe right-sided lateral pleuritic chest pain lasting a few minutes. In the private hospital emergency room, chest radiography and computed tomography (CT) had shown pleural masses, which were subsequently found to be poorly differentiated epithelial mesothelioma.
The patient reported that, over the previous week, she had felt weak and lethargic, but was otherwise well. She had no previous serious illnesses, but had recently started taking iron supplements for anaemia and occasionally took non-steroidal anti-inflammatory agents for osteoarthritis. She was a non-drinker, and had ceased smoking 5 months previously. (She started smoking at the age of 16 years and had been smoking 40 cigarettes a day.) She was a widow with three adult children, and had emigrated from the United Kingdom in 1969. Her husband died at the age of 39 years of a myocardial infarction. Her father died of carcinoma of the oesophagus, and her mother of “old age”. Her four siblings and three adult children were all well.
Although she had no history of asbestos exposure from any of her husband’s occupations, she could have been exposed to asbestos during two periods of her life. From the age of 15–22 years in the UK, she worked as a machinist in a factory where asbestos lagging was used for the steam pipes of steam presses and central heating. Then, in 1984, her son worked for a year for a company making asbestos gaskets, and throughout this period she washed his work overalls.
On examination, she looked well and was not in pain. She weighed 74 kg and was of normal build, but had slight conjunctival pallor. An electrocardiogram showed sinus rhythm; her blood pressure was 140/60 mmHg, and her jugular venous pressure was not elevated. There was no cyanosis or clubbing. Examination of the chest, cardiovascular system, breast, abdomen and peripheries showed no abnormalities.
Investigations
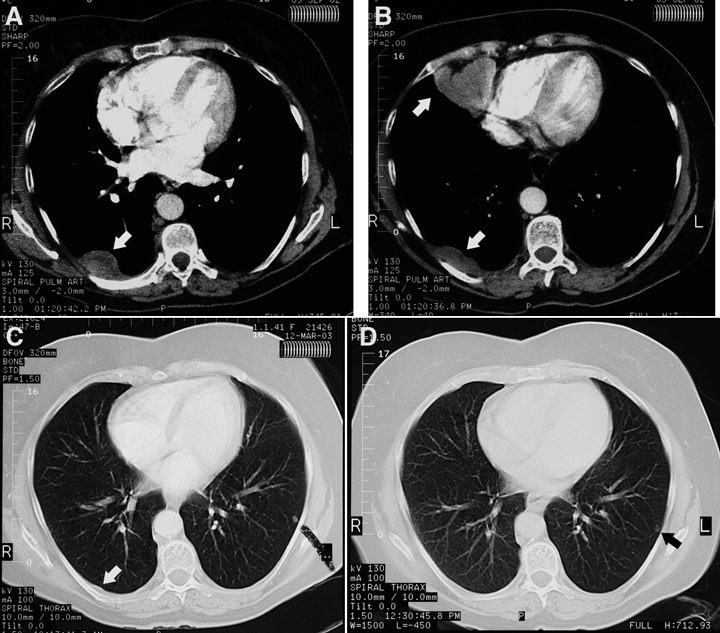
A chest radiograph taken before referral showed a pleural density measuring 10 cm × 2 cm overlying the posterior aspect of the right lower lobe, with no pleural plaques or other stigmata of asbestos exposure. A CT pulmonary angiogram performed the same day to exclude pulmonary embolism showed three pleural masses in the right side of the chest — the first corresponding to the opacity visible on the chest radiograph in the right costovertebral gutter at the level of the tracheal bifurcation, the second having a diameter of 6 cm and located in the right cardiophrenic angle (not of fatty attenuation), and the third in the right posteromedial costophrenic recess, just above the diaphragm (Box 1A and Box 1B). The lungs, mediastinum and upper abdomen (including the pancreas and para-aortic nodes) were normal.
Laboratory tests showed her haemoglobin level was 104 g/L (reference range [RR], 115–160 g/L), with a normochromic normocytic anaemia; she had thrombocytosis (555 × 109/L [RR, 150–450 × 109/L]) and leukocytosis (11.2 × 109/L [RR, 4.0–11.0 × 109/L]), with mild neutrophilia (8.2 × 109/L [RR, 2.0–7.5 × 109/L]). Her erythrocyte sedimentation rate was markedly elevated at 110 mm/h (RR, 1–30 mm/h), as was her serum C-reactive protein level (294 mg/L [RR, 0–6 mg/L]). She had mildly elevated concentrations of liver enzymes (alanine aminotransferase, 98 U/L [RR, 0–45 U/L]; aspartate aminotransferase, 70 U/L [RR, 0–41 U/L]; and lactate dehydrogenase, 268 U/L [RR, 80–250 U/L]), with normal serum bilirubin and alkaline phosphatase levels. Her serum iron level was low (2 μmol/L [RR, 10–33 μmol/L]).
A core biopsy (20 mm × 1 mm) of one of the right pleural masses showed morphological and immunohistochemical features of a poorly differentiated epithelial mesothelioma. A pathology report by an experienced pathologist with a special interest in pulmonary and pleural pathology read:
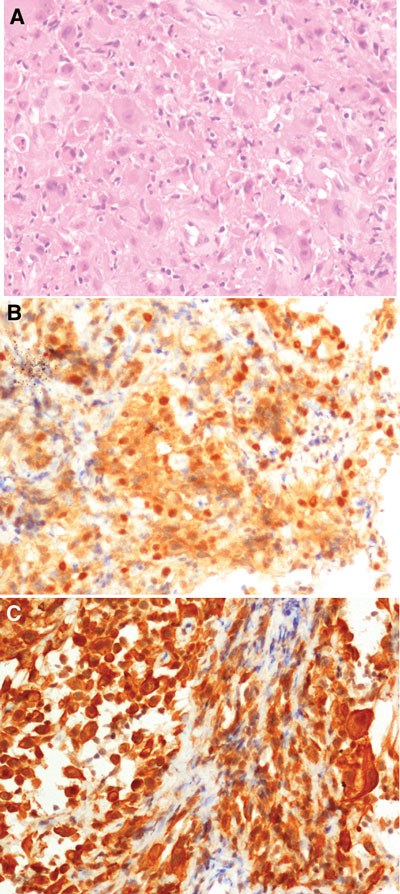
There is a proliferation of poorly cohesive large cells many of which had vesicular nuclei, prominent nucleoli and abundant eosinophilic cytoplasm. Occasional binucleate and multinucleate forms are present and there is a small amount of associated collagenous stroma with a mild chronic inflammatory cell infiltrate [Box 2A]. There is no evidence of mucin production, and immunoperoxidase stains for a variety of keratins are strongly positive, along with positive staining for calretinin [Box 2B] and cytokeratin 5/6, both markers of mesothelial differentiation [Box 2C]. Stains for LCA and S100 protein are negative.
The pathology results were later reviewed by another pathologist with considerable experience of mesothelioma, who drew the same conclusion.
Management
The patient was told the diagnosis and referred to an oncologist with a special interest in mesothelioma in another tertiary hospital where clinical trials of drugs for the treatment of mesothelioma were in progress. She was offered chemotherapy and entry in a thalidomide trial, but, by the time she was entered, the tumour was already showing signs of spontaneous regression.
The patient opted for no treatment, as she felt well. By 30 December 2002, a repeat CT scan of the chest showed a decrease in the size of the large, right-sided pleural mass in the costovertebral gutter from 17 mm × 9 mm (CT chest scan, 29 November 2002) to 12 mm × 6 mm. The second pleural mass was now so small it was difficult to see. The third mass was not visible, and there were two small intrapulmonary nodules — one in the right middle lobe and the other in the left lower lobe. By March 2003, the first and second pleural masses were even smaller (Box 1C) and, by June 2003, they had disappeared (Box 1D). A CT chest scan in June 2004 was normal except for the two tiny intrapulmonary nodules that had not changed in size and were probably granulomas. The patient was last reviewed in June 2007 and was in good health, with no evidence of tumour, and was scheduled for next review in 6 months.
Discussion
There have been a few reports of spontaneous regression of malignant mesothelioma, but prolonged, disease-free periods are rare. Our report appears to be the first to describe a patient in Australia with a poorly differentiated, multifocal epithelial mesothelioma that regressed spontaneously, with the disease remaining in remission for 5 years.
There has been one case report of a patient with malignant mesothelioma of the pleura that regressed spontaneously, but after 6 years there was a single recurrence, which was resected surgically, and the patient was followed up for a total of 12 years.1 This raises the question in such cases of the duration of follow-up. In the latter case, a prominent host response to tumour was seen in both the primary tumour and the recurrence. In another case, a patient had a spontaneous remission of a malignant peritoneal mesothelioma, and had high spiking fevers when the tumour recurred.2
A report from Western Australia described a woman whose tumour regressed spontaneously but who eventually died 20 months later.3 It was noted that the tumour tissue was infiltrated with mononuclear cells, and as the tumour recurred some malignant mesothelioma antigens disappeared.
Several aspects of our case should be noted.
Histopathology
The histopathological findings for our patient’s tumour were re-examined by another pathologist.
Not all three lesions were biopsied, as it was felt highly probable that the pathological findings for all three would be identical.
Author’s experience
I have considerable experience in the management of mesothelioma and benign asbestos-related conditions and currently see about 600 patients with this condition a year. I also act as an expert witness for the courts.
Mesothelioma is a relatively common condition in Australia at present and, as a result, our thoracic physicians, oncologists and pathologists have considerable experience in this area.
Course of the disease
The patient had markedly elevated inflammatory markers and is likely to have had the tumour for several months before diagnosis. It is suspected that her natural killer cells and cell-mediated immunity accounted for the regression of the tumour.
Evidence of the beginning of spontaneous regression was unusually rapid, occurring within months of diagnosis.
Exposure
Our patient’s exposure to asbestos seems to have been relatively mild and incidental, as often occurs with women who develop mesothelioma.
Self-treatment
The patient did not use any unusual therapies, such as alternative medicines, diets and faith healing, after the diagnosis.
This case highlights the possibility that spontaneous regression of mesothelioma may occur occasionally. Spontaneous tumour regression therefore should be seen as part of the spectrum of the natural history of mesothelioma and other tumours. A detailed study of the immunity of such individuals “after the event” is unlikely to reveal any particular abnormality but, in hindsight, it would have been interesting to have performed detailed immunological studies during the initial regression period. The role of mesothelin-related serum proteins needs further evaluation. The understanding of this process is likely to be pivotal in the improved treatment of this usually lethal condition.
1 Computed tomography (CT) scans of the chest at referral (September 2002) and 6 and 9 months later
2 Histological examination of a core biopsy specimen from one of the pleural masses (Box 1)
 |
|
A: Histological section of the core biopsy of the pleural mass in Box 1A showing sheet-like proliferation of pleomorphic epithelioid cells with abundant eosinophilic cytoplasm, representing a poorly differentiated epithelioid malignant mesothelioma. B: Core biopsy showing a positive result on immunoperoxidase staining for calretinin. C: Core biopsy showing a positive result on immunoperoxidase staining for cytokeratin 5/6. |
Competing interests
None identified.
Acknowledgements
I would like to thank Dr Rick Abraham, Medical Oncologist and Senior Lecturer in Medicine, University of Queensland, for his assistance in the management of this patient; Dr Ian LeFevre, Histopathologist, QML Pathology, Brisbane, and Dr Lyndie Clark, Histopathologist, Prince Charles Hospital, Brisbane, for reviewing the histological sections; and Dr Ian LeFevre and QML Pathology for supplying the photomicrographs.
References
- Pilling JE, Nicholson AG, Harmer C, Goldstraw P. Prolonged survival due to spontaneous regression and surgical excision of malignant mesothelioma. Ann Thorac Surg 2007; 83: 314-315. 0_i1091901
- Schwartz E, Maayan C, Mouallem M, et al. Malignant peritoneal mesothelioma: long-term spontaneous clinical remission. Med Pediatr Oncol 1991; 19: 325-328. 0_i1091903
- Robinson BW, Robinson C, Lake RA. Localised spontaneous remission in mesothelioma — possible immunological mechanism. Lung Cancer 2001; 32: 197-201. 0_i1091906