




Syncope is a transient and abrupt loss of consciousness and postural tone that is generally followed by rapid recovery without the need for a major intervention. It is due to a transient reduction in cerebral blood flow, is frequently related to posture, and is the most common cause of transient loss of consciousness. Syncope has a lifetime cumulative incidence of 35%2 and accounts for 1%–2% of all emergency department visits.3,4 Morbidity, even from “benign” causes of syncope, is profound: 70% of people experiencing recurrent syncope suffer impairment to activities of daily living, 6% suffer fractures, 64% restrict their driving and 39% change employment.5-7 Recurrent syncope can have a major impact on quality of life, with devastating psychosocial consequences similar to those associated with other chronic diseases.6,7
Syncope can be classified into three categories: cardiac syncope, non-cardiac syncope and syncope of undetermined cause (Box 1). Patients with cardiac syncope have the highest mortality rate and need prompt evaluation. However, the majority of patients fall into the non-cardiac syncope category — the most challenging form of syncope to investigate and manage. Most of these patients have a disorder of postural circulatory control (Box 2), the mechanism of which is poorly understood. The diagnosis and treatment of this patient group is the major focus of our clinical update.
Postural syncope has a bimodal distribution in the general population. The first peak, at around 15 years, predominates in girls, with the vast majority of cases being due to vasovagal syncope.3 In the second peak, at over 60 years, vasovagal syncope, orthostatic hypotension and situational syncope (eg, during micturition or after meals) are predominant, but clinical presentations are often diverse, posing a diagnostic challenge. Cardiac syncope remains a major culprit in this age group and must be excluded.
The important question of whether a patient has cardiac syncope must always be answered and, in the majority of cases, this can be done with a thorough history and electrocardiography. In patients under 40 years of age with no known cardiac disease, no symptoms suggestive of cardiac disease, no family history of sudden death at a young age, no experience of syncope during exercise, and a completely normal electrocardiogram (ECG), the probability of cardiac syncope is extremely low.8,9 Patients over 60 years of age tend to have more atypical presentations and are more likely to have occult heart disease.10 Strong consideration should be given to more aggressive investigations in this age group. It is worth noting that about 50% of patients with syncope and heart disease have a non-cardiac cause of syncope.9
We recognise five clinical phenotypes of postural syncope:
Vasovagal syncope;
Postural tachycardia syndrome (POTS);
Autonomic failure;
Persistently low supine systolic blood pressure; and
Initial orthostatic hypotension.
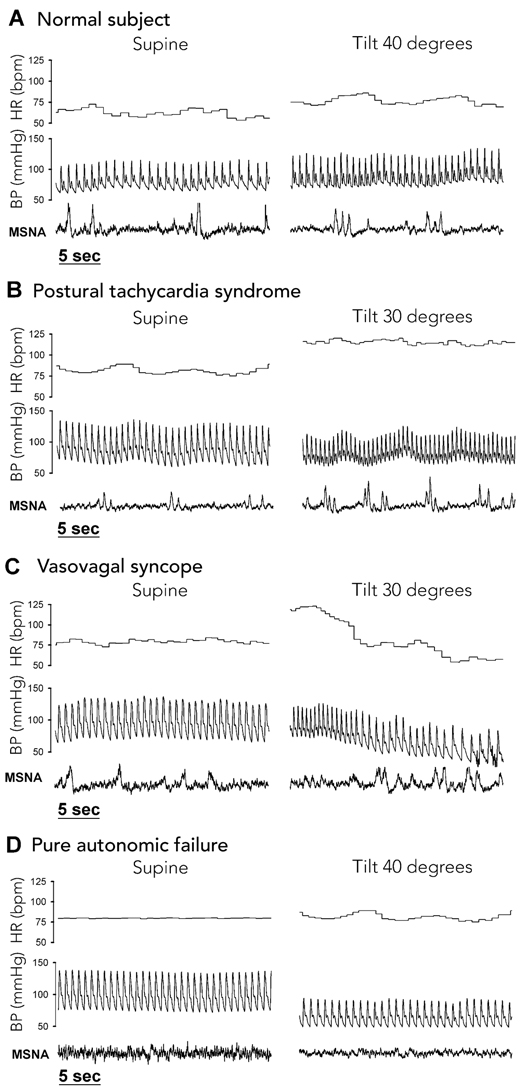
Vasovagal syncope is a common and clinically challenging disorder widely recognised in the lay community as a faint or “blackout”. It is characterised physiologically by sudden hypotension and varying degrees of bradycardia (Box 3). The mechanism remains a matter of controversy. Excess venous pooling and abnormal vasodilation while standing, thus reducing venous return to the heart, is the most commonly accepted explanation. Vasovagal syncope is classically provoked by prolonged standing or sitting. However, other stimuli may be operative in “situational” syncope (eg, in response to venepuncture, pain or emotion). Most patients can be diagnosed by careful history taking,12 examination and electrocardiography. Symptoms consistent with vasovagal syncope and most predictive of the diagnosis include visual blurring, sweating, nausea, warmth, light-headedness and fatigue.10,13 Palpitations are also a common feature of the prodrome. A third of patients have no warning symptoms.14 Young patients tend to present with typical features, while older patients more commonly have an atypical presentation. A brief convulsion is quite common, and mild seizure activity due to cerebral hypoperfusion may occur in up to two-thirds of patients.15 It has been estimated that about 20% of patients undergoing long-term follow-up in hospital epilepsy clinics are misdiagnosed — their transient loss of consciousness being due to syncope rather than epileptic seizure.15 Tilt-table testing may be needed to confirm a suspected diagnosis of vasovagal syncope. The key is in correlating symptoms on the tilt table with those in the real world.
POTS is a perplexing condition that has only been recently identified in the medical literature.16 The disorder, which most commonly affects young women, is characterised by fatigue, palpitations, exercise intolerance, light-headedness, visual blurring, chest pain, inability to concentrate and episodic syncope or presyncope (ie, the sensation that fainting may occur without actual syncope).16 Anxiety and depression are frequent comorbidities. A hallmark of this condition is that, during syncope, blood pressure is maintained or only falls minimally, while heart rate increases dramatically (Box 3). An increase in heart rate of at least 30 beats/min after 10 minutes of standing, or a heart rate of > 120 beats/min with prolonged standing, is suggestive of the diagnosis. The onset of POTS is often abrupt and, in about 50% of cases, follows a minor infection. POTS appears to be a manifestation of sympathetic nervous system hyperactivity17 during standing and is the subject of ongoing research by our group.
Chronic autonomic failure is an uncommon but important group of conditions that cause orthostatic intolerance. Syndromes of chronic autonomic failure include pure autonomic failure (PAF) (degeneration of sympathetic nerves), multiple system atrophy (MSA) (degeneration of the central nervous system), diabetic autonomic neuropathy and Parkinsonism with autonomic failure. Autonomic failure clinically manifests as progressive fatigue and orthostatic intolerance. Other features include erectile dysfunction, urinary retention, loss of sweating, pain in the neck and shoulders, abdominal discomfort and diarrhoea. Supine hypertension is common, with a substantial postural drop in blood pressure upon standing and absent reflex tachycardia. The onset of PAF is typically in the fifth or sixth decade of life, and men are affected twice as often as women. In PAF there is degeneration of the sympathetic nerves, including those in the heart, producing near-total sympathetic denervation.18
MSA, on the other hand, is a central nervous system deterioration. Clinically, MSA has cerebellar signs, Parkinsonian signs or mixed signs. It is a progressive disorder that usually results in death 7–10 years after onset. This is in stark contrast to PAF, in which long-term survival is the norm. Differentiating MSA with Parkinsonian signs from Parkinson’s disease can be difficult. However, Parkinson’s disease tends to respond more favourably to levodopa treatment and shows patchy sympathetic denervation on myocardial scintigraphy using 123I-metaiodo-benzylguanidine.19
Persistently low supine systolic blood pressure is not emphasised in the medical accounts of postural syncope but was recognised in a large syncope trial.4 In general, the medical view is that low “normal” blood pressure is healthy, protecting against the development of cardiovascular disease. However, some patients with frequent presyncope or syncope have systolic blood pressures of 85–100 mmHg on a “good day”. Systolic blood pressure can easily fall to 80 mmHg as a result of minimal dehydration or drinking a small amount of alcohol. In clinical practice we find this to be a common cause of syncope — patients frequently complain of ongoing fatigue and may also have a prominent tachycardia during orthostasis, which can make differentiation from POTS difficult. Our preliminary data suggest that these patients have low resting sympathetic activity as the basis of their low blood pressure and are prone to vasovagal events.
Initial orthostatic hypotension is a common cause of presyncope and syncope immediately (5–10 s) after standing up. A clear history of the immediacy of symptoms is the cornerstone of diagnosis. It occurs most often after prolonged recumbency or after squatting. Initial orthostatic hypotension is defined physiologically as an exaggerated transient fall in blood pressure of > 40 mmHg (systolic) and/or 20 mmHg (diastolic) within 15 seconds of standing up.20 This contrasts with typical orthostatic hypotension that occurs within 3 minutes of standing and may be delayed for up to 10 minutes after standing. Continuous beat-to-beat blood pressure monitoring is required for a physiological diagnosis, but this diagnostic method has a high false-negative rate.20 Initial orthostatic hypotension is common in young adults,21 with an incidence of 3.6%.2
Various guidelines have been published for evaluating syncope.8,9,22,23 Our preferred diagnostic algorithm is shown in Box 4. The recent consensus statement of the American Heart Association and the American College of Cardiology Foundation23 is primarily useful for providing a diagnostic path for excluding cardiac causes of syncope associated with sudden death. It does not address diagnosis and management of postural syncope and is neglectful of the clinical importance of disorders of circulatory control.24
Taking a detailed history is the most powerful tool for diagnosing syncope. Measuring supine and standing blood pressures is crucial: typical orthostatic hypotension is characterised by a fall in blood pressure of > 20 mmHg (systolic) and/or 10 mmHg (diastolic) after 3 minutes of standing. It is also important to test blood pressure after prolonged standing (10 minutes), as delayed hypotension is common.25 The absence of reflex tachycardia on standing suggests autonomic failure.
For cardiovascular investigations, a 12-lead ECG is essential (Box 5). It may identify arrhythmias or preconditions for arrhythmia (eg, a long QT interval) or indicate underlying ischaemic heart disease. An abnormal ECG has prognostic value. Yet despite its obvious clinical importance, only 59% of patients with syncope presenting to US emergency departments in 2004 were given an ECG at presentation.26
External loop recorders, which may be worn for 1 month, require patient activation when symptoms occur. They increase diagnostic yields to 25%,27 but problems with dermal electrode tolerance and forgetting to trigger recording at the onset of symptoms limit their effectiveness.28
Implantable loop recorders are inserted under the skin of the chest wall, requiring only local anaesthetic. A recent study of patients with at least three severe episodes of neurally mediated syncope (orthostatic hypotension excluded) demonstrated the value of early loop recorder implantation and subsequent guided therapy.29
Electrophysiological testing in cases of unexplained syncope remains controversial and is limited to select patients, usually those with structural heart disease.8
Tilt-table testing is a widely used method for evaluating postural syncope. It is predominantly used to diagnose vasovagal syncope. It may also be used to train patients to recognise the vasovagal prodrome — some patients can then abort a vasovagal event using counter-manoeuvres such as leg-crossing.30 The diagnosis should only be made if the event during tilt-table testing reproduces the patient’s real-world event. The use of tilt-table testing remains controversial:31 publications report a wide range of sensitivity and specificity, with lack of specificity being a particular problem. The use of provocation testing with isoprenaline is of questionable merit32 — it is possible to induce vasovagal syncope in almost anyone with an adequately aggressive tilt test. In a patient with a normal ECG, structurally normal heart, no neurological features, normal supine blood pressure and a negative tilt test, vasovagal syncope is still the likely diagnosis.
At the Baker Heart Research Institute we perform invasive tilt testing. This involves cardiac monitoring and placement of an arterial line for blood pressure monitoring. We routinely determine whole-body spillover of noradrenaline to plasma, as a neurochemical measure of sympathetic nervous system activity.33 Microneurography, measuring sympathetic nerve firing in fibres passing to skeletal muscle blood vessels, is performed using a fine tungsten electrode placed in the peroneal nerve.34 The response to orthostasis measured using these two techniques provides important complementary diagnostic information for many causes of unexplained postural syncope (Box 3).
Therapy for disorders of circulatory control (Box 6) is based on limited randomised trial data. Evidence for many aspects of treatment is restricted to small observational series and case reports. Our treatment recommendations are based on limited available data, referenced where appropriate, but based also on our clinical experience.
Treatment centres on education, awareness of precipitants, and staying safe. Avoiding dehydration, carrying a water bottle (with the target of keeping urine clear), and increasing salt intake are beneficial. Lower-body muscle tensing35 and physical manoeuvres such as leg-crossing30 are effective and evidence-based.
Treatment with fludrocortisone, a highly selective mineralocorticoid, may reduce the frequency of attacks by expanding intravascular volume through salt and water retention. The drug is the subject of an ongoing clinical trial.36 Pressor agents such as midodrine may be effective: limited randomised trial data support therapy with midodrine for selected patients (under the Therapeutic Goods Administration Special Access Scheme).37 Beta-blockers have long been advocated to treat vasovagal syncope, but a recently published syncope prevention trial investigating metoprolol versus placebo in 206 patients showed no benefit.38 Reboxetine, a noradrenaline transporter inhibitor used for depression, may be helpful and has been shown to prolong the time taken to faint during head-up tilt testing in healthy subjects.39
Cardiac pacing has been studied in several clinical trials, with mixed results. Overall, the evidence does not support pacemaker insertion as first-line therapy — for example, the second vasovagal pacemaker study, a randomised, double-blinded trial of 100 patients with severe vasovagal syncope, failed to show a reduction in vasovagal events.40
Treatment of POTS is challenging. Education and psychosocial support are critical; adequate hydration41 and increased salt intake may help. Mineralocorticoids, such as fludrocortisone in low doses,42 or natural liquorice may reduce the frequency of events. Pressor agents have mixed success and there is great variability in patients’ response to treatment.41,43 Acetylcholinesterase inhibitors reduce tachycardia and appear to benefit some patients.44 Beta-blockers may help reduce palpitations but rarely help syncope, which may get worse. Selective serotonin reuptake inhibitors may be beneficial.5 Anecdotally, calcium channel blockers in low doses have proved useful, presumably by reducing cerebral vasospasm, which is thought to be the basis of postural syncope occurring in the absence of postural hypotension.
Therapy for orthostatic intolerance includes fluids, salt intake, fludrocortisone and pressor agents. Direct-acting α-adrenergic agonists such as dihydroergotamine45 or midodrine46 are most useful in PAF, but are also of use in MSA. Erythropoietin improves orthostatic tolerance in patients with autonomic failure and may be considered when other agents are ineffective.47 Supine hypertension is common and can be severe, often requiring bedtime dosing with short-acting antihypertensives such as hydralazine.48
Treatment revolves around education and limiting precipitants. No therapy has been studied systematically, but it is sensible to recommend getting up slowly and sitting for a short time before standing, and it is logical to encourage fluid and salt intake. Immediate bending over to lower the head after standing, followed by a gradual return to normal posture, may reduce cerebral hypoperfusion. Wieling et al advocate the tensing of leg muscles immediately after standing to abort hypotensive events.20
2 Aetiology of syncope and transient loss of consciousness
Low cardiac output/pump failure:
Disorders of circulatory control:
Vasovagal syncope
Postural tachycardia syndrome
Autonomic failure
Persistently low supine systolic blood pressure
Initial orthostatic hypotension
Other disorders (relating to drugs, hypovolaemia, anaemia)
3 Diagnostic profiles in postural syncope during invasive head-up tilt testing*
4 Evaluation of syncope*
 | |||||||||||||||
|
ECG = electrocardiogram. * Adapted from European Society of Cardiology recommendations.9 | |||||||||||||||
- Gautam Vaddadi1
- Elisabeth Lambert1
- Susan J Corcoran2
- Murray D Esler1
- 1 Baker Heart Research Institute, Melbourne, VIC.
- 2 Cardiac Investigation Unit, St Vincent’s Hospital, Melbourne, VIC.
We thank the National Health and Medical Research Council (NHMRC) and National Heart Foundation for continued funding of our research. Gautam Vaddadi is the recipient of a cofunded Postgraduate Research Scholarship, Elisabeth Lambert is the recipient of an NHMRC Career Development Award, and Murray Esler is a Senior Principal Research Fellow of the NHMRC.
None identified.
- 1. Engel GL. Psychologic stress, vasodepressor (vasovagal) syncope, and sudden death. Ann Intern Med 1978; 89: 403-412.
- 2. Ganzeboom KS, Mairuhu G, Reitsma JB, et al. Lifetime cumulative incidence of syncope in the general population: a study of 549 Dutch subjects aged 35–60 years. J Cardiovasc Electrophysiol 2006; 17: 1172-1176.
- 3. Colman N, Nahm K, Ganzeboom KS, et al. Epidemiology of reflex syncope. Clin Auton Res 2004; 14 Suppl 1: 9-17.
- 4. Mathias CJ, Deguchi K, Schatz I. Observations on recurrent syncope and presyncope in 641 patients. Lancet 2001; 357: 348-353.
- 5. Grubb B, Olshansky B, editors. Syncope: mechanisms and management. 2nd ed. Malden, Mass: Blackwell Futura, 2005.
- 6. Linzer M, Pontinen M, Gold DT, et al. Impairment of physical and psychosocial function in recurrent syncope. J Clin Epidemiol 1991; 44: 1037-1043.
- 7. van Dijk N, Sprangers MA, Colman N, et al. Clinical factors associated with quality of life in patients with transient loss of consciousness. J Cardiovasc Electrophysiol 2006; 17: 998-1003.
- 8. Brignole M, Alboni P, Benditt D, et al. Task force on syncope, European Society of Cardiology. Part 2. Diagnostic tests and treatment: summary of recommendations. Europace 2001; 3: 261-268.
- 9. Brignole M, Alboni P, Benditt D, et al. Task force on syncope, European Society of Cardiology. Part 1. The initial evaluation of patients with syncope. Europace 2001; 3: 253-260.
- 10. Colman N, Nahm K, van Dijk JG, et al. Diagnostic value of history taking in reflex syncope. Clin Auton Res 2004; 14 Suppl 1: 37-44.
- 11. Morillo CA, Eckberg DL, Ellenbogen KA, et al. Vagal and sympathetic mechanisms in patients with orthostatic vasovagal syncope. Circulation 1997; 96: 2509-2513.
- 12. Sheldon R, Rose S, Connolly S, et al. Diagnostic criteria for vasovagal syncope based on a quantitative history. Eur Heart J 2006; 27: 344-350.
- 13. Calkins H, Shyr Y, Frumin H, et al. The value of the clinical history in the differentiation of syncope due to ventricular tachycardia, atrioventricular block, and neurocardiogenic syncope. Am J Med 1995; 98: 365-373.
- 14. Grubb BP. Clinical practice. Neurocardiogenic syncope. N Engl J Med 2005; 352: 1004-1010.
- 15. Zaidi A, Clough P, Cooper P, et al. Misdiagnosis of epilepsy: many seizure-like attacks have a cardiovascular cause. J Am Coll Cardiol 2000; 36: 181-184.
- 16. Grubb BP, Kosinski DJ, Boehm K, et al. The postural orthostatic tachycardia syndrome: a neurocardiogenic variant identified during head-up tilt table testing. Pacing Clin Electrophysiol 1997; 20: 2205-2212.
- 17. Goldstein DS, Holmes C, Frank SM, et al. Cardiac sympathetic dysautonomia in chronic orthostatic intolerance syndromes. Circulation 2002; 106: 2358-2365.
- 18. Goldstein DS, Holmes C, Cannon RO 3rd, et al. Sympathetic cardioneuropathy in dysautonomias. N Engl J Med 1997; 336: 696-702.
- 19. Courbon F, Brefel-Courbon C, Thalamas C, et al. Cardiac MIBG scintigraphy is a sensitive tool for detecting cardiac sympathetic denervation in Parkinson’s disease. Mov Disord 2003; 18: 890-897.
- 20. Wieling W, Krediet CT, van Dijk N, et al. Initial orthostatic hypotension: review of a forgotten condition. Clin Sci (Lond) 2007; 112: 157-165.
- 21. Ganzeboom KS, Colman N, Reitsma JB, et al. Prevalence and triggers of syncope in medical students. Am J Cardiol 2003; 91: 1006-1008, A8.
- 22. Brignole M, Alboni P, Benditt DG, et al. Guidelines on management (diagnosis and treatment) of syncope — update 2004. Executive summary. Eur Heart J 2004; 25: 2054-2072.
- 23. Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF Scientific Statement on the evaluation of syncope: from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation: in collaboration with the Heart Rhythm Society: endorsed by the American Autonomic Society. Circulation 2006; 113: 316-327.
- 24. Benditt DG. The ACCF/AHA Scientific Statement on Syncope: a document in need of thoughtful revision. Clin Auton Res 2006; 16: 363-368.
- 25. Gibbons CH, Freeman R. Delayed orthostatic hypotension: a frequent cause of orthostatic intolerance. Neurology 2006; 67: 28-32.
- 26. Sun BC, Emond JA, Camargo CA Jr. Inconsistent electrocardiographic testing for syncope in United States emergency departments. Am J Cardiol 2004; 93: 1306-1308.
- 27. Linzer M, Pritchett EL, Pontinen M, et al. Incremental diagnostic yield of loop electrocardiographic recorders in unexplained syncope. Am J Cardiol 1990; 66: 214-219.
- 28. Sivakumaran S, Krahn AD, Klein GJ, et al. A prospective randomized comparison of loop recorders versus Holter monitors in patients with syncope or presyncope. Am J Med 2003; 115: 1-5.
- 29. Brignole M, Sutton R, Menozzi C, et al. Early application of an implantable loop recorder allows effective specific therapy in patients with recurrent suspected neurally mediated syncope. Eur Heart J 2006; 27: 1085-1092.
- 30. van Dijk N, Quartieri F, Blanc JJ, et al. Effectiveness of physical counterpressure maneuvers in preventing vasovagal syncope: the Physical Counterpressure Manoeuvres Trial (PC-Trial). J Am Coll Cardiol 2006; 48: 1652-1657.
- 31. Sheldon R. Tilt testing for syncope: a reappraisal. Curr Opin Cardiol 2005; 20: 38-41.
- 32. Kapoor WN, Brant N. Evaluation of syncope by upright tilt testing with isoproterenol. A nonspecific test. Ann Intern Med 1992; 116: 358-363.
- 33. Esler M, Willett I, Leonard P, et al. Plasma noradrenaline kinetics in humans. J Auton Nerv Syst 1984; 11: 125-144.
- 34. Lambert E, Hotchkin E, Alvarenga M, et al. Single-unit analysis of sympathetic nervous discharges in patients with panic disorder. J Physiol 2006; 570: 637-643.
- 35. Krediet CT, van Dijk N, Linzer M, et al. Management of vasovagal syncope: controlling or aborting faints by leg crossing and muscle tensing. Circulation 2002; 106: 1684-1689.
- 36. Raj SR, Rose S, Ritchie D, et al. The Second Prevention of Syncope Trial (POST II) — a randomized clinical trial of fludrocortisone for the prevention of neurally mediated syncope: rationale and study design. Am Heart J 2006; 151: 1186, e11-17.
- 37. Kaufmann H, Saadia D, Voustianiouk A. Midodrine in neurally mediated syncope: a double-blind, randomized, crossover study. Ann Neurol 2002; 52: 342-345.
- 38. Sheldon R, Connolly S, Rose S, et al. Prevention of Syncope Trial (POST): a randomized, placebo-controlled study of metoprolol in the prevention of vasovagal syncope. Circulation 2006; 113: 1164-1170.
- 39. Schroeder C, Birkenfeld AL, Mayer AF, et al. Norepinephrine transporter inhibition prevents tilt-induced pre-syncope. J Am Coll Cardiol 2006; 48: 516-522.
- 40. Connolly SJ, Sheldon R, Thorpe KE, et al. Pacemaker therapy for prevention of syncope in patients with recurrent severe vasovagal syncope: Second Vasovagal Pacemaker Study (VPS II): a randomized trial. JAMA 2003; 289: 2224-2229.
- 41. Jacob G, Shannon JR, Black B, et al. Effects of volume loading and pressor agents in idiopathic orthostatic tachycardia. Circulation 1997; 96: 575-580.
- 42. Freitas J, Santos R, Azevedo E, et al. Clinical improvement in patients with orthostatic intolerance after treatment with bisoprolol and fludrocortisone. Clin Auton Res 2000; 10: 293-299.
- 43. Hoeldtke RD, Bryner KD, Hoeldtke ME, et al. Treatment of postural tachycardia syndrome: a comparison of octreotide and midodrine. Clin Auton Res 2006; 16: 390-395.
- 44. Raj SR, Black BK, Biaggioni I, et al. Acetylcholinesterase inhibition improves tachycardia in postural tachycardia syndrome. Circulation 2005; 111: 2734-2740.
- 45. Olver IN, Jennings GL, Bobik A, et al. Low bioavailability as a cause of apparent failure of dihydroergotamine in orthostatic hypotension. BMJ 1980; 281: 275-276.
- 46. Low PA, Gilden JL, Freeman R, et al. Efficacy of midodrine vs placebo in neurogenic orthostatic hypotension. A randomized, double-blind multicenter study. Midodrine Study Group. JAMA 1997; 277: 1046-1051.
- 47. Hoeldtke RD, Streeten DH. Treatment of orthostatic hypotension with erythropoietin. N Engl J Med 1993; 329: 611-615.
- 48. Shibao C, Gamboa A, Diedrich A, et al. Management of hypertension in the setting of autonomic failure: a pathophysiological approach. Hypertension 2005; 45: 469-476.
Abstract
Postural syncope is a transient loss of consciousness secondary to a reduction in cerebral blood flow and is typically precipitated by standing. It is the commonest cause of recurrent transient loss of consciousness.
Recurrent unexplained postural syncope is most often due to one of the five disorders of circulatory control: vasovagal syncope, postural tachycardia syndrome, chronic autonomic failure, initial orthostatic hypotension, or persistently low supine systolic blood pressure.
Failure to identify the underlying cause of postural syncope can result in ongoing morbidity, impaired quality of life and high health care costs.
With a detailed history, examination, blood pressure assessment and electrocardiography, most disorders of circulatory control can be diagnosed.
In difficult cases, analysis of sympathetic nervous system and circulatory responses during head-up tilting can aid diagnosis.
Treatment is challenging and compounded by a lack of evidence. Most patients can be managed in an outpatient setting, and hospital admission or emergency department assessment is rarely warranted.