





Volume 184 - Issue 10
Emphysematous pyelonephritis
Authors: John V Peter, Vishwanath Biradar and Sandra L Peake
Med J Aust 2006; 184 (10): 533. || doi: 10.5694/j.1326-5377.2006.tb00356.x
Published online: 15 May 2006
Published online: 15 May 2006
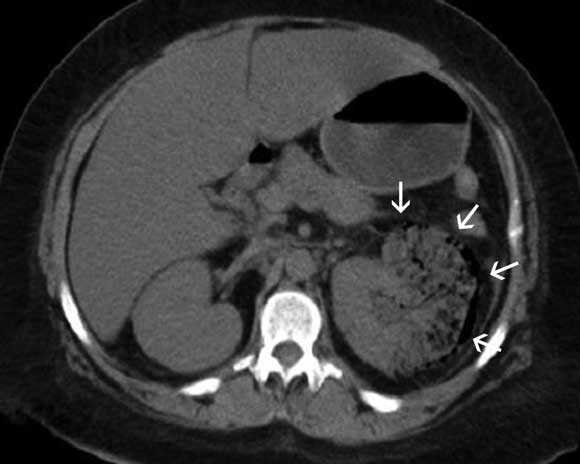
A 40-year-old Indigenous woman with type 2 diabetes presented with a 6-month history of intermittent left flank pain. She reported worsening pain of 2 days’ duration associated with fever, nausea, vomiting and reduced urine output. Clinical examination revealed tenderness over the left loin. An x-ray (not shown) and computed tomogram of the abdomen (Box) suggested a diagnosis of emphysematous pyelonephritis.
Over the next few hours, the patient developed septic shock. In view of the severity of the emphysematous pyelonephritis, as evidenced by the extent of gas in the renal system on imaging and the development of septic shock, an urgent laparotomy and left nephrectomy were performed. Escherichia coli was isolated from blood cultures and from tissue of the necrotic kidney. After surgery and with antibiotic treatment, the woman made a slow recovery.
Emphysematous pyelonephritis is a rare, severe gas-forming infection of the renal parenchyma, typically seen in people with diabetes. Radiologically, four classes of emphysematous pyelonephritis are described on computed tomography:1 in Class 1 and 2, the gas is localised to the collecting system and the renal parenchyma, respectively, without extension to the extrarenal space; in Class 3A, as seen in this case, there is extension of gas or abscess into the perinephric space, and in Class 3B, to the pararenal space; bilateral emphysematous pyelonephritis or emphysematous pyelonephritis of a solitary kidney represents the most severe form of the disease (Class 4).
Emphysematous pyelonephritis is associated with a high mortality rate (40%) when treated with antibiotics alone.1 Although milder forms of the disease (Class 1 and 2) have been successfully treated with a combination of percutaneous drainage and antibiotics, these modalities alone may not be sufficient in more severe presentations of the disease or in patients presenting with septic shock. In such patients, early nephrectomy is recommended.1,2
Competing interests
None identified.
References
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med 2000; 160: 797-805. 0_i1091773
- Adbul-Halim H, Kehinde EO, Abdeen S, et al. Severe emphysematous pyelonephritis in diabetic patients: diagnosis and aspects of surgical management. Urol Int 2005; 75: 123-128. 0_i1091777