





Volume 183 - Issue 7
Electronic medical handover: towards safer medical care
Authors: Lean-Peng Cheah, Debbie H Amott, James Pollard and David A K Watters
Med J Aust 2005; 183 (7): 369-372. || doi: 10.5694/j.1326-5377.2005.tb07086.x
Published online: 3 October 2005
Published online: 3 October 2005
Abstract
As the working hours of junior doctors decrease, adequate handover of patients becomes more important to maintain continuity of care and avoid errors caused by information gaps.
A minimum dataset for surgical handover should include the patient’s name, location (ward and bed number), date of admission, diagnosis, procedure (with date), complications and progress, management plan, resuscitation plan, consultant availability (and instructions if not available), expected need for review, and name of doctor completing handover and date to confirm that information is current.
An electronic handover system is a potential solution, but our survey shows that free-text entry into such systems may be inadequate; prompts or predefined fields for handover content are possible solutions.
Junior doctors in hospitals cannot work 24 hours a day, 7 days a week. When they go off-duty, some form of information handover to the relieving team is necessary to ensure continuity of care. With the moves to reduce junior doctors’ working hours, the number of handovers is increasing. However, the quality of handovers can be poor.1 Lack of information when a patient needs urgent and often unexpected care is a clinical risk. In addition, as on-call periods are often busy, a handover system that identifies the patients most in need of review and the required decisions would assist doctors in setting priorities.
Suggestions to improve the quality of handovers include electronic handovers,2,3 and the development of guidelines for hand-overs.4 Guidelines are also endorsed by the Australian Safety and Quality Council in Health Care.5
In our hospital, the impetus to document and improve hand-overs arose from a root-cause analysis of a surgical adverse event in late 2003. A patient died of septicaemia complicating peritonitis caused by a leaking large-bowel anastomosis. The cause of the patient’s deteriorating condition was not initially recognised, and the patient died despite a late repeat laparotomy. The deterioration occurred over a weekend when communication between the on-call doctors and the specialist responsible for care could have been improved. Although our hospital, like many others, assumed that handovers take place, there were no formal policies or guidelines about what information should be included in handover.
We describe the process of developing an improved, electronic handover system for junior doctors at our hospital, a regional teaching hospital with 400 beds.
Developing a minimum dataset for handover
In early 2004, we reviewed handover procedures for surgical patients at the hospital. In consultation with junior and senior doctors and the Clinical Risk Management Committee, we determined the data and functions required for electronic handover and handback. Handover needs to inform about the patient’s location and unit, the consultant normally responsible for care, diagnosis, length of stay, procedures, and plan or instructions for the handover period (Box 1).
In addition, we defined the required functions for an electronic handover system. The system should be able to:
Print a patient list for the specialty or units being covered;
Sort the list by ward and bed number, by consultant, by unit, or by need for review;
Allow handover information to be entered efficiently (ideally with a single mouse click); and
Allow patients from other specialties (eg, a medical unit) for whom consultations have been requested to appear in the “patients-to-review” list.
Developing an electronic handover system
Many of the required data were already present in the two electronic information systems in use in the hospital. The CORDis system (Correspondence, Operation notes, Reports and Discharge summaries) was used hospital-wide to generate discharge summaries, clinic letters, operation notes, audit reports and drug prescriptions. CORDis (http://www.cordisehr.com.au) was developed by Dynamic Solutions (Melbourne, Vic; www.dynamic.net.au) in association with Barwon Health, and introduced in 2001, with the Pharmaceutical Benefits Scheme prescribing function added in early 2002.
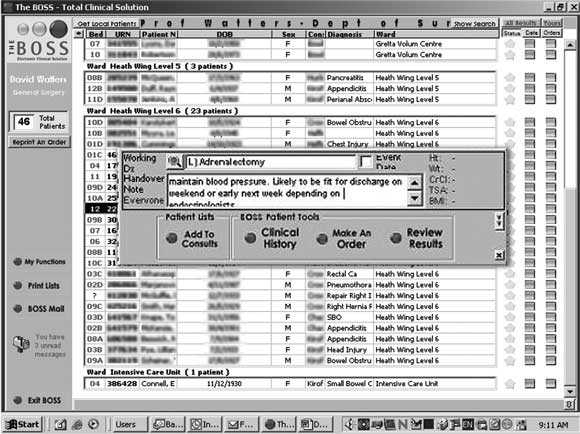
In addition, the review of handover procedures coincided with the roll-out of a second information system, the BOSS (Core Medical Solutions, Adelaide, SA; www.coremedicalsolutions.com). This system was used for reporting results of laboratory investigations, and through linking to the radiology reporting system it provided a common system for reporting all investigation results. The BOSS system also includes a free-text window for recording handover information if desired. The system creates lists of patients with location, diagnosis, length of stay, recent results and any content inserted in the free-text window (Box 2).
In 2004, neither system was able to provide all the required handover information. In devising a solution, our guiding principles were to avoid duplication of data entry and to ensure that information viewed was accurate and up-to-date. Our initial approach was to build fields for the minimum dataset into CORDis, as we had easy access to its developers. We did not attempt to replicate the transmission of investigation results into CORDis, as this would have been complex and expensive. The handover system was available in CORDis with more predefined fields for content (Box 1) but without investigation results, and in the BOSS with a free-text field for data entry. The inclusion of laboratory results on the tasklists generated by the BOSS meant that it became the preferred system for junior doctors to use during ward rounds and handover.
Evaluating the BOSS handover system
As junior doctors preferred to use the BOSS system for handovers, we investigated the adequacy of the BOSS free-text entries for communicating the minimum dataset for general surgery patients. Our hospital has four general surgical units and one vascular unit, each staffed on weekdays by one registrar and one resident medical officer. On weekends and public holidays, responsibility for all five units is handed over to one on-call registrar and one resident, the latter changing on the second and any subsequent days.
We reviewed the BOSS general surgery on-call handover sheets (comprising the combined lists of the four general surgical and one vascular unit) for 14 weekends and public holidays in 2004 and between December 2004 and February 2005. The aim was to determine the total number of patients for whom the on-call junior doctor was responsible, and the number of patients with no handover information entered.
In addition, we conducted a prospective survey of registrars and residents receiving handovers and those receiving handback on seven consecutive weekends and public holidays between December 2004 and February 2005. For each handover, the on-call registrar and resident were interviewed by one of the authors (D A K W) and given an evaluation form to complete. This form asked about the completeness and usefulness of the handover information. Results from the registrar, as the team leader, were scored, except in the case of opinions about the desirability of electronic handover. The registrars receiving handback were also interviewed about events, discharges and discharge summaries and any problems.
Results are shown in Box 3. On average, completing the handover information took 10 minutes, for seven to eight patients per unit, while completing handback information took 2 minutes per event for 2–3 events per unit during the on-call period (2 discharges and 0–1 other event).
The need for handovers and the value of a documented handover was universally accepted by junior doctors. Doctors volunteered that they were particularly pleased with the ability of the BOSS to include results of recent laboratory tests on a handover sheet, which encouraged use of the system.
We found that the system reliably identified patients and their locations. However, the free-text entry, although helpful, was often deficient in particular information, such as decisions that needed to be made in ward rounds and consultant availablity. In addition, handback information was not completed consistently, particularly when patients were discharged or transferred to another unit (eg, from a surgical to a medical unit). We found a documented handback in only half the patients with significant events. While almost 80% of doctors returning to duty were informed of patients who had been discharged, only 13% knew whether a discharge summary had been done.
The BOSS handover procedure was also used on an ad-hoc basis by junior doctors in other clinical services. Handover for medical patients could take twice as long as for surgical patients, as they often have multiple problems, each problem with its own therapeutic intervention, instead of a single procedure.
Discussion
We found that that free-text entries in an electronic system were not adequate to convey all the information required for a thorough patient handover. Handover information needs to identify a list of patients and their location, to highlight their priority for review, and indicate the availability of the treating specialist. A system to provide this information is relatively simple to develop if a clinical information system is already in place. However, it is more complex to ensure that the system updates, while also retaining a copy of “who, what and when” entered the handover information should it ever be necessary to review the information conveyed. A further challenge is to ensure that any system being developed is used. If a handover system is to be successfully implemented, it needs to be seen as advantageous by its users — simple, informative, time-saving and practical.
In our hospital, the information required for handovers by junior doctors originated in two separate electronic systems. The situation is probably similar in many other Australian hospitals. To be simple and effective, and to avoid duplication of data entry, all hospital systems need to be linked so that all necessary information can be presented in one handover list. We considered two potential solutions:
To replicate what was wanted from one of the systems into the other (a short-term, interim solution).
To develop a web browser that could access both systems and build handover preferences on an HTML page (a longer-term solution). A web-based system could be introduced in two phases: a first read/print-only phase; and a second phase permitting data entry.
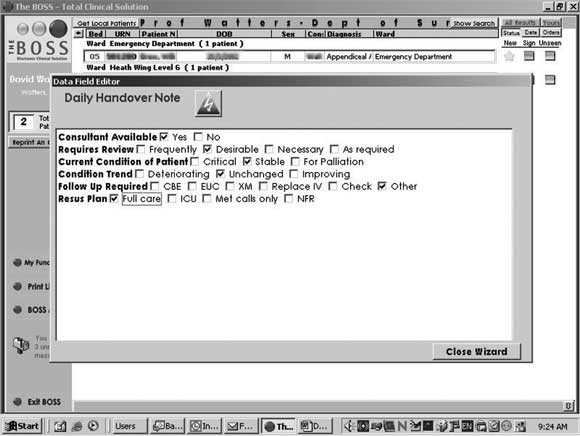
We are currently developing the second solution. The ability to view handover information on a personal digital assistant would also be a significant attraction of such a system.6 In the meantime, we have developed a “handover wizard” in the BOSS system to prompt for required handover information from junior doctors who choose to use it (Box 4).
Other hospitals can use the dataset we have identified (Box 1) to develop their own handover solutions. Each hospital needs to determine where the necessary information resides in their electronic systems and to devise a local solution for presenting it in a single screen or patient list.
Continuity of care is important to patients but must be balanced against junior doctors’ working hours and the dangers of fatigue. Recent studies have shown that reducing working hours decreases attentional failures and medical errors.7,8 In Australia, the average working week has dropped from over 100 hours to under 70 hours in recent times, as errors caused by fatigue have become unacceptable.9,10 A surgical registrar is now rarely on a 1 day in 2 on-call roster, with 1 day in 4 or 5 being the norm. Thus, handover information must be provided on 75%–80% of working days. Senior staff are also becoming increasingly less available — particularly on weekends — as they arrange cover through group practices or take long weekend breaks.
Similar changes are being implemented overseas. In the United Kingdom, the European Working Time Directive limits doctors in training to 48 hours’ work a week.11,12 This weekly limit is being implemented in stages, with an interim average 58-hour working week. A “hospital at night” project is looking at specific issues in regard to the increased number of shifts, competency and hand-over.13,14 In the United States, the Accreditation Council for Graduate Medical Education has also recently limited duty hours for medical residents to 80 hours per week.15
We believe further research and evaluation are required to fine tune the format of handover for different medical specialties and to demonstrate the effectiveness of introducing formal handover systems into other hospitals.
1 A minimum data set for handover
Generated automatically from hospital information system
Patient (name, UR no.)
Patient age
Date of admission/day of stay
Patient location (ward and bed number)
Consultant responsible for care
Treating unit
Current diagnosis
Results of recent investigations
To be entered by junior doctor going off duty
Handover note (free text)
Update current diagnosis
Recent procedure(s) and date(s)
Desirable (or required in a free-text note)
Consultant availability
Insurance status*
Need for and urgency of review†
Patient’s condition‡
Condition trend§
Management plan¶
Resuscitation plan**
Investigations pending/required
Name of doctor completing handover information
Date of handover update
* Insurance status (private or public) to help determine whether changes in patient’s condition should be reported to the patient’s private consultant rather than the on-call team.
†We recommend a drop down menu with choices: frequently, necessary, desirable, as required.
‡We recommend a drop down menu with choices: critical (unstable), stable, for palliation.
§We recommend a drop down menu with choices: improving, deteriorating, unchanged.
¶Management plan (eg, remove drain tube, discharge, resume normal diet).
** Resuscitation plan (eg, full resuscitation, not for life support, MET
[medical emergency team] calls only, not for resuscitation).
2 The BOSS electronic system with free-text handover
Screen shot from the BOSS handover system showing the free-text field used to enter a handover note. This field is brought up by clicking on the patient row.
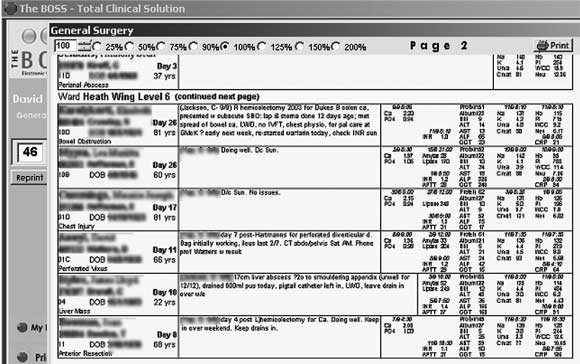
Screen shot showing the “Print a tasklist” format which contains the handover information (central section), laboratory results (right hand section) and patient name, age, length of stay, diagnosis and consultant in charge (left hand section).
3 Survey of the adequacy of the BOSS free-text handover system
Question |
Response |
||||||||||||||
Handover |
|
||||||||||||||
Average number of patients to hand over (n = 14) |
7–8 |
||||||||||||||
Average time taken to fill in handover information (min) (n = 14) |
10 |
||||||||||||||
Is it a good idea to fill in a formal electronic handover? (Yes [%]) |
7/7 (100%) |
||||||||||||||
The weekend round |
|
||||||||||||||
Average number of patients doctor is responsible for (n = 7) |
40 |
||||||||||||||
Average number with incomplete handover information (n = 7) |
8 (20%) |
||||||||||||||
Did you know where your patients were? (Yes [%]) |
7/7 (100%) |
||||||||||||||
Did you know what was wrong with your patients? (Yes [%]) |
5/7 (71%) |
||||||||||||||
Did you know what decisions had to be made? (Yes [%]) |
4/7 (57%) |
||||||||||||||
Did the handover list help remind you of key investigations to do/results to review? (Yes [%]) |
6/7 (85%) |
||||||||||||||
Was information about consultants’ availability adequate? (Yes [%]) |
3/7 (41%) |
||||||||||||||
Is an electronic handover system desirable?* (Yes [%]) |
14/14 (100%) |
||||||||||||||
Handback |
|
||||||||||||||
Were the handover data updated over the weekend for handback? (Yes [%]) |
7/14 (50%) |
||||||||||||||
Does the handover system identify significant events that happened while you were off-duty? (Yes [%]) |
8/13 (61%)† |
||||||||||||||
Do you know who was discharged or died while you were away? (Yes [%]) |
11/14 (79%) |
||||||||||||||
Do you know if the discharge summaries were done? (Yes [%]) |
2/14 (13%) |
||||||||||||||
* Denominator was 14 as replies were scored from both registrar and resident. † Denominator was 13 as no significant events occurred on one weekend. |
|||||||||||||||
References
- Roughton VJ, Severs MP. The junior doctor handover: current practices and future expectations. J R Coll Physicians Lond 1996; 30: 213-214. 0_i1091735
- Volpp KGM, Grande D. Residents’ suggestions for reducing errors in teaching hospitals. N Engl J Med 2003; 348: 851-855. 0_i1091737
- Young RJ, Horsley SD, McKenna M. The potential role of IT in supporting the work of junior doctors. J R Coll Physicians Lond 2000; 34: 366-370. 0_i1091739
- Junior Doctors Committee. Annual report 2004. London: British Medical Association, 2004. Available at: http://www.bma.org.uk/ap.nsf/Content/jdcannualreport2004 (accessed Mar 2005).
- Australian Safety and Quality Council in Health Care. Safe staffing — discussion paper. Canberra: Safety and Quality Council, 2003. Available at: http://www.safetyandquality.org/articles/Publications/SafeStaffing_web.pdf (accessed Dec 2004).
- Wilcox RA, La Tella RR. The personal digital assistant: a new medical instrument for the exchange of clinical information at the point of care. Med J Aust 2001; 175: 659-662. 0_i1091745
- Lockley SW, Cronin JW, Evans EE, et al. Effect of reducing interns’ weekly hours on sleep and attentional failures. N Engl J Med 2004; 351: 1829-1837. 0_i1091747
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med 2004; 351: 1838-1848. 0_i1091749
- Australian Medical Association (Victoria). Australian Medical Association (Victoria) Hospital Medical Officer Certified Agreement 2002. Melbourne: AMA, 2002. 0_i1091751
- Nocera A, Khursandi DS. Doctors’ working hours: can the medical profession afford to let the courts decide what is reasonable? Med J Aust 1998; 168: 616-618. 0_i1091753
- Phillips H, Morris PJ. The Royal College of Surgeons of England and the European Working Time Directive – a policy statement. London: RCS, 2003. Available at: http://www.rcseng.ac.uk/publications/docs/ewtd_policy_statement.html/view?searchterm=European%20Working%20Time%20Directive (accessed Dec 2004).
- British Medical Association. Time’s up 1 August 2004. A guide on the EWTD for junior doctors. London: BMA, 2004. Available at: http://www.bma.org.uk/ap.nsf/Content/TimesUp/$file/TimesUp2.pdf (accessed Dec 2004).
- NHS Modernisation Agency. The hospital at night. Report and recommendations of the hospital at night project. Available at: http://www.modern.nhs.uk/workingtime/17048/WhatisHospitalatNight/1_1.pdf (accessed Feb 2005).
- MacDonald R, Eccles S. The hospital at night. BMJ Career Focus 2004; 328: 19; doi:10.1136/bmj.328.7431.s19. Available at: http://careerfocus.bmjjournals.com/cgi/content/full/328/7431/s19 (accessed Mar 2005).
- Common program requirements (resident duty hours). Chicago: Accreditation Council for Graduate Medical Education, 2003. Available at: http:// www.acgme.org/acWebsite/dutyHours/dh_dutyHoursCommonPR.pdf (accessed Dec 2004).
Getting on the Same Page: Why Australia Needs a National Maternity Early Warning System (MEWS) Chart
Briony A. Cutts, Lucy Bowyer, Nisha Khot, Sandra Lowe, Stefan C. Kane
Data for Equity: Can Linked Administrative Data Inform Pathways to More Equitable Child Health?
Sarah Gray, Shuaijun Guo, Meredith O'Connor, Elodie O'Connor, Katrina Williams, Hannah Badland, Susan Woolfenden, Josie Dickerson, Gerry Redmond, Marnie Downes, Sharon R. Goldfeld
Specialty College Selection: Why Change is Critical to Support a Future Rural Workforce
Matthew R. McGrail, Jenny May AM, Katherine Logan
The number of cancer‐related deaths that could be attributable to spatial disparities in survival in Australia, 2010–2019: a retrospective population‐based cohort study
Charlotte K Bainomugisa, Jessica Cameron, Paramita Dasgupta, Peter Baade
Differentiated and simplified oral HIV pre‐exposure prophylaxis (PrEP) models hold the key to virtually eliminating HIV transmission in Australia by 2030
Tyson Arapali, Sarah Warzywoda, Anthony K J Smith, Curtis Chan, Timothy R Broady, Erin Sullivan, Catherine MacPhail, Mohamed A Hammoud, Alexander Dowell‐Day, Benjamin R Bavinton
Non‐technical errors associated with deaths in surgical care, Australia, 2012–2019, by surgical specialty (Australian and New Zealand Audit of Surgical Mortality): a retrospective cohort study
Jesse Ey, Victoria Kollias, Octavia Lee, Kelly Hou, Matheesha Herath, John B North, Ellie Treloar, Suzanne Edwards, Martin Bruening, Adam J Wells, Guy J Maddern