





Volume 182 - Issue 2
A case of desquamating rash associated with methadone use
Authors: Natalie Kordjian, Annabelle D Donaldson, Steven A Krilis and Dedee F Murrell
Med J Aust 2005; 182 (2): 76-77. || doi: 10.5694/j.1326-5377.2005.tb06580.x
Published online: 17 January 2005
Published online: 17 January 2005
A man who had been taking prescribed methadone for many years presented with a desquamating rash (predominantly affecting the hands and feet) complicated by cellulitis of the right leg. There have now been multiple reports of a similar rash among methadone users in Sydney. The cause remains unknown.
We report a man attending a methadone program in south-east Sydney who presented with a distinctive rash complicated by lower-leg cellulitis. This case adds to the widespread reports of a similar rash in methadone users around Sydney. The cause is under investigation by the New South Wales Department of Health.
Clinical record
In October 2004, a middle-aged man was referred to a hospital in south-east Sydney with a 14-day history of a painful, swollen, erythematous right lower leg and fever. Two days before onset of the leg symptoms, he had noticed a non-pruritic rash which started on his legs and feet and spread to abdomen and arms; it was accompanied by swelling, and then desquamation of the hands and feet. He had been diagnosed with cellulitis of the right lower leg 7 days before presentation and was prescribed oral flucloxacillin, but his condition did not improve significantly. Duplex ultrasound examination of the right leg 2 days before presentation excluded deep vein thrombosis. He was admitted to hospital for intravenous antibiotic treatment.
The patient was a former intravenous heroin user and had been in a methadone program at a local pharmacy for the previous 8 years. He denied recreational drug use or injecting or sharing the oral methadone. His past medical history included previous right-leg deep vein thrombosis, chronic hepatitis B and C infection, gastro-oesophageal reflux, as well as melanoma excision several years before, and cholecystectomy a month previously. He had been taking griseofulvin for about 3 months for onychomycosis.
He was taking methadone syrup (160 mg daily), griseofulvin (500 mg daily) and, when required, diazepam (5 mg three times daily), codeine/paracetamol (30/500 mg three times daily) and oxycodone (40 mg twice daily). He had recently started using, when required, cyproheptadine (4 mg at night), hyoscine (20 mg four times daily) and triamcinolone acetonide (0.02% cream topically) for the rash, and metoclopramide (10 mg three times daily) for mild nausea.
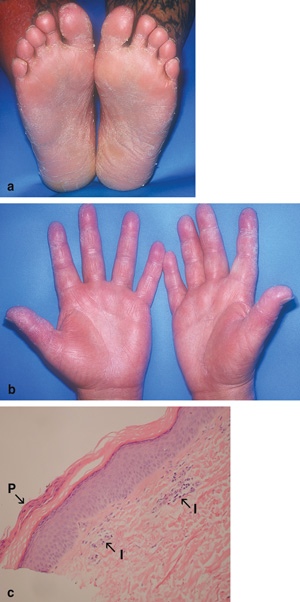
On physical examination, the patient was haemodynamically stable and looked well. His temperature was 37.2°C. There was erythema, tenderness and warmth below the right knee, consistent with cellulitis. There was desquamation of the skin of both his lower legs, soles of feet (Box, a) and palms and fingers (Box, b), as well as non-pitting oedema of the feet and hands. There was hyperkeratosis of the soles, with xerosis and an erythematous maculopapular rash of the arms. The skin condition did not appear typical of disorders causing hyperkeratosis and desquamation, which usually do not present concurrently. He had no mucosal ulceration. Differential diagnoses included the early phase of an exfoliative erythroderma, psoriasis triggered by infection, early pityriasis rubra pilaris, bacterial toxin-mediated exfoliation, viral exanthem, sarcoidosis and syphilis.
Rash in a patient who used oral methadone
A: Hyperkeratosis and desquamation of the soles of the feet. B: Desquamation of the palms. C: Biopsy specimen from the maculopapular rash on the left arm, showing a slightly thickened epidermis with focal parakeratosis (P), and mild perivascular lymphocytic infiltrate (I). (Original magnification, × 20; haematoxylin–eosin stain.)
Measurement of serum electrolyte, urea and creatinine levels and liver function tests all gave normal results. A full blood count revealed haemoglobin level of 125 g/L (reference range [RR], 130–180 g/L) and slight eosinophilia (0.48 × 10 9/L; RR, 0.04–0.44 × 10 9/L), but total white cell count was within the reference range (6.2 × 109/L; RR, 3.5–11.0 × 10 9 /L). Erythrocyte sedimentation rate was 10 mm/h (RR, 1–10 mm/h) and C-reactive protein level was 24 mg/L (RR, < 3 mg/L). Blood cultures showed no growth. A test for Treponema pallidum antibody was negative. Chest x-ray was normal, and HIV antibody test negative.
Skin biopsy of the red macules on his left arm (Box, c) and the right-leg biopsy revealed non-specific histological changes, suggestive of chronic dermatitis. Periodic acid–Schiff staining for fungi was negative.
Empirical treatment was begun with mometasone cream (0.1%), calcipotriol ointment (0.005%) and sorbolene cream twice daily to affected areas, and coal tar (5%) and salicylic acid (5%) in sorbolene base cream at night to the feet. Intravenous cephazolin (1 g three times daily) and oral clindamycin (300 mg four times daily) were begun for the cellulitis.
The patient was discharged on Day 4 with the above topical preparations and oral cephalexin (500 mg three times daily), after both the rash and right-leg cellulitis abated significantly. He failed to attend a follow-up appointment, but reported by telephone that the rash had gradually resolved over several weeks.
Discussion
This case raises the alert to a possible adverse reaction to a methadone preparation. The cause may be methadone itself, another component of the preparation, or a contaminant. Previously reported cutaneous reactions to methadone include angioedema, facial oedema, flushing, pruritus, purpura, rash and urticaria.1 To our knowledge, no cases have been reported of a desquamating rash associated with methadone or other opioids.
The cause of the rash in our patient did not appear infectious. He had no clinical evidence of staphylococcal toxic shock syndrome; he remained clinically well and did not develop the diffuse confluent erythema typical of this syndrome. Nor was the rash typical of a viral exanthem, in which a widespread morbilliform eruption predominates, without confluent erythema (as occurred on the lower legs), hyperkeratosis or desquamation. A reaction to a medication other than methadone seems less likely, as there had been no recent change.
We are aware of other patients with a similar rash, oedema and desquamation of the hands and feet, all taking methadone: six patients in a methadone program at the same pharmacy as our patient, 20 from a local methadone clinic, and others at other methadone centres in Sydney (Mary Anne Ford, Registered Nurse, Bayside Clinic, Sydney, NSW, personal communication). We know of no patient with a similar rash who is not using methadone, and we believe all affected patients were taking the same brand and formulation of the drug. Most cases have been mild, and close contacts have not been affected. All patients appear to have continued using methadone from their usual dispensing clinic, and the rash has resolved over several weeks.
The cause of the reaction remains unknown, and is possibly even an illicit drug available on the street. However, as all affected patients appear to have been taking methadone, this is perhaps the most likely agent. Marijuana has been reported, albeit rarely, to cause allergic reactions, and occasionally becomes contaminated with biological or chemical substances that might cause a reaction.2 -4 However, in that situation, one would expect cases to be more widely distributed outside the methadone-using population. In addition, at least one client with this rash from the local methadone clinic had a negative urine test for cannabinoids (Mary Anne Ford, as above, personal communication).
Further investigation of these cases is required to determine the aetiology. Variables to be considered include the brand and batch of methadone used, storage, dose, mixing of batches in the dispensing pump, and other solutions included in the preparation to increase palatability. Pharmacists often mix batches of methadone and are not required to record the batch number dispensed to each patient, which makes tracing difficult. Also important to consider are any other prescription or non-prescription medications taken by patients, illicit drugs used, and sharing of methadone between patients from different methadone clinics.
Many more cases may have been unreported and unrecognised, as most affected patients have had relatively mild and self-limiting symptoms. An investigation is now under way by the New South Wales Department of Health. Methadone clinics, pharmacists, dermatologists, general practitioners and emergency medicine staff need to be aware of the possibility of these reactions.
Competing interests
None identified.
Acknowledgements
We acknowledge the assistance of the Bayside Clinic, Sydney, NSW, and Dr Kim Tran, Department of Anatomical Pathology, St George Hospital, Sydney, NSW.
References
- Litt J, Pawlak WA. Methadone. In: Litt J, Pawlak WA. Drug eruption reference manual. New York: Parthenon Publishing Group, 1997: 271. i1085703
- Liskow B, Liss JL, Parker CW. Allergy to marihuana. Ann Intern Med 1971; 75: 571-573. i1085705
- Kagen SL. Aspergillus: an inhalable contaminant of marihuana. N Engl J Med 1981; 304: 483-484. pgfId-1085707
- Taylor DN, Wachmuth IK, Yung-Hui S, et al. Salmonellosis associated with marijuana. N Engl J Med 1982; 306: 1249-1253. i1085708