





Volume 182 - Issue 12
A community-based intervention to reduce antibiotic use for upper respiratory tract infections in regional South Australia
Authors: William B Dollman, Vanessa T LeBlanc, Lynette Stevens, Peter J O’Connor and John D Turnidge
Med J Aust 2005; 182 (12): 617-620. || doi: 10.5694/j.1326-5377.2005.tb06847.x
Published online: 20 June 2005
Published online: 20 June 2005
Abstract
Objective: To evaluate the effectiveness of a community-based and GP-based intervention in reducing unnecessary antibiotic prescribing for upper respiratory tract infections (URTIs) including sore throats, sinusitis and otitis media.
Design: Analysis of pharmacy dispensing data in June to October before (2000) and after (2001) the intervention, which commenced on 25 June 2001.
Setting and participants: Local consumers, health professionals, the Adelaide Southern Division of General Practice, the South Australian Government, and the local media in a rural region of South Australia, covering about 2000 square kilometres, with a population of over 20 000.
Intervention: Community dissemination of consumer information on antibiotic use for URTIs (including a local media campaign) and education of health professionals (including sessions with general practitioners at the four practices in the study area) on current Australian therapeutic guidelines for antibiotics, and a validated clinical scoring system for decision making in managing sore throat.
Main outcome measures: Total dispensing data from local pharmacies for the months of June to October in 2000 and 2001, covering the six antibiotics considered most likely to be used for URTIs (amoxycillin, amoxycillin/clavulanic acid, cefaclor, doxycycline, erythromycin and roxithromycin).
Results: The dispensing of the six antibiotics reduced by 32% overall, from 77.1 to 52.9 defined daily doses per 1000 population per day, with statistically significant reductions in the range of 31%–70% for individual antibiotics; there was no reduction for amoxycillin with or without clavulanic acid.
Conclusion: The intervention was associated with reduced dispensing of unnecessary antibiotics for URTIs.
In 1999, the Joint Expert Technical Advisory Committee on Antibiotic Resistance (JETACAR) reported that current levels of antibiotic prescribing raise serious concerns about the indiscriminate use of these agents — particularly in the primary health care setting — and subsequent risks of emerging bacterial resistance.1
It is now accepted that there is minimal benefit of treating patients with self-limiting conditions such as sore throats, sinusitis, acute bronchitis and acute otitis media, and no demonstrated need for antibiotic treatment of uncomplicated upper respiratory tract infections (URTIs).2 Antibiotics can cause side-effects, and prescribing them reinforces patients’ belief that antibiotics are necessary.2
Prescribing antibiotics has been identified as one of the most uncomfortable prescribing decisions made by doctors in general practice.3 Doctors’ perceptions of patient pressure and diagnostic uncertainty contribute greatly to the decision-making process.4,5
A range of evidence-based strategies have been shown to significantly reduce the unnecessary prescribing of antibiotics. “Educational marketing” techniques directed towards health care professionals,6,7 the use of scoring systems by general practitioners,8 patient information leaflets and delayed prescriptions9 have all been shown to optimise antibiotic prescribing in primary health care. Parent education has been considered the single most important element in reducing oral antibiotic overuse in children.10
Australia’s National Strategy for the Quality Use of Medicines11 advocates measures such as those listed above, and also identifies the need for activities to raise awareness, develop knowledge and skills, and reinforce existing behaviours that support quality use of medicines, recognising that more limited approaches do not lead to sustained behaviour change.
We decided to trial an intervention aimed at reducing antibiotic prescribing for URTIs through education programs aimed at prescribers and consumers by using the clinical sore throat score of McIsaac et al,8 and to compare antibiotic prescribing during the winter of 2001 (the intervention period) with prescribing during the previous winter. This approach to managing patients with an upper respiratory tract infection and sore throat has been shown to be useful in community-based family practice,12 and could substantially reduce the unnecessary prescribing of antibiotics for these conditions.
Methods
The study was carried out in part of the Southern Fleurieu Peninsula of South Australia, an area of about 2000 square kilometres with a mixture of rural and beachside towns. At the time of the study, the area had a population of over 20 000 with 25 GPs in four practice locations, and five pharmacies. The area is about one and a half hours’ drive from Adelaide, and has been the site of a Quality Use of Medicines (QUM) initiative (the QUM Coast) involving local health professionals and the community, to promote non-drug options for managing insomnia.13
Ethical approval for the study was granted by the Ethics of Research Committee of the University of South Australia.
The intervention
Pamphlets were prepared for patients, highlighting the risks and benefits of antibiotic use in managing URTIs in the community. These were distributed to general practices, pharmacies, the local hospital, primary schools, childcare centres, clubs and the Community Health Service from 25 June to October 2001. An article appeared in the local community newspaper on 12 July.
We conducted education sessions for GPs in the four practices on the QUM Coast in late June 2001, with expert clinical input by one of the authors (J T). Sessions were based on material in the Therapeutic guidelines: antibiotic,14 and covered the management of URTIs generally, and the specific use of the sore throat scoring system. The separate score sheet (Box 1) was prepared for use by the doctors in assessing the possibility of streptococcal infection as a cause of sore throat, and provided guidance on the use of antibiotics. In some surgeries, the practice nurses determined the score with the patient or their parents before the consultation. This process facilitated discussions with the patient on diagnosis and treatment options, raising general awareness of the broader issues of antibiotic use for URTIs.
The antibiotics
An assessment was made of the antibiotics most likely to be prescribed for URTIs. The Therapeutic guidelines: antibiotic14 recommended penicillin V or roxithromycin for sore throat, amoxycillin, cefaclor, doxycycline or amoxycillin/clavulanic acid for sinusitis, and amoxycillin, amoxycillin/clavulanic acid or cefaclor for otitis media. Erythromycin was recommended for pertussis. Pharmaceutical Benefits Scheme dispensing data for 2000 showed amoxycillin (4 485 000 prescriptions), roxithromycin (2 549 000), amoxycillin/clavulanic acid (2 516 000), cefaclor (1 941 000), doxycyline (1 764 000), and erythromycin (1 024 000) to be the six most commonly prescribed antibiotics overall.15 There were 686 000 prescriptions for penicillin V in the same period.
Data analysis
At the end of the intervention, total dispensing data (including non-subsidised medicines) related to the prescribing of the six antibiotics were collected from the five pharmacies in the area for the period 1 June to 31 October in the years 2000 and 2001. Data were entered into an Access database16 and transferred to SPSS17 for analysis and an Excel18 spreadsheet for reporting. Dispensing rates were reported as defined daily doses per 1000 population per day.
Demographic data were obtained for the project region and for the Australian population from the Australian Bureau of Statistics 2001 census.19
Results
A total of 5660 pamphlets were distributed during the intervention period. Initially, 1000 copies of the clinical sore throat score sheet were distributed to GP practices, but demand for additional copies resulted in a further 1600 being distributed.
Population demographic data (Box 2) showed a greater percentage of people over the age of 50 and fewer under the age of 30 in the study area compared with the Australian population.
Box 3 shows dispensing data and the percentage change in total dispensing between the preproject and project periods for each drug. There was an overall reduction in dispensing between these periods of 32%, and this was statistically significant (Mann–Whitney U, < 1; P < 0.01). Individually, there was a statistically significant change in dispensing between the preproject and project periods (P < 0.01) for each antibiotic except amoxycillin and amoxycillin/clavulanic acid.
Doxycycline is used for URTIs, but also for acne, bronchiectasis, pelvic inflammatory disease and urethritis. Under the assumption that packs of seven tablets or capsules were being used for URTIs and larger packs for chronic conditions, we assessed the change in dispensing volume for the small pack sizes separately. This showed a statistically significant 49% reduction in dispensing volume (Mann–Whitney U, < 1; P < 0.01); this was a larger reduction than the 31% decrease for all pack sizes of doxycycline.
Discussion
After the intervention, there was a statistically significant and substantial reduction in the dispensing of nearly all of the antibiotics considered most likely to be used for URTIs. While reductions in dispensing could reflect general reductions in antibiotic use for all indications in the study region, or causes other than the intervention, at least some of the decrease was likely to be a direct consequence of the intervention.
Dispensing data for total antibiotics (Box 3) suggest an association with a winter illness, such as URTI, raising confidence that the antibiotics are being used for such a condition. Also, there was a greater decrease in dispensing of the small packs of doxycycline, suggesting a stronger impact of the intervention on the pack size most likely to have been prescribed for URTIs.
State and national trends for the selected antibiotics (9% and 6% reductions, respectively)20 were not statistically significant: (Mann–Whitney U, 8 and 7; P = 0.42 and P = 0.31, respectively), so there was a substantially greater impact in the study region. If the state and national trends can be taken as indicative of the impact of the nation-wide National Prescribing Service (NPS) campaigns at the time,21,22 it could be interpreted that the QUM Coast intervention substantially enhanced their impact.
The intervention had no effect on the prescribing of amoxycillin, with or without clavulanic acid. It may be that the NPS thrust to reduce prescribing of amoxycillin for URTIs had the desired effect, and that there was no further room for improvement. The NPS reported that the prescribing of amoxycillin declined substantially before the year 2000.21 It is also possible that by the time of the intervention, perhaps as a consequence of NPS campaigns, amoxycillin was mostly being prescribed for other indications so the impact of the intervention might not have been measurable for this antibiotic.
The decision to use complete dispensing data, collected from local pharmacy dispensing computer systems, rather than relying on data from the PBS, was based on an assessment of local dispensing data before the study, which showed that only 60%–65% of antibiotic prescriptions in the region were eligible for subsidy under the PBS (unpublished). However, we found a lack of consistency between pharmacy software systems and their ability to generate reports in a convenient way, which would limit the ability to conduct a larger evaluation without committing significant resources to this method of data collection.
There were some limitations to our study. We collected prescription data for all antibiotic use and not just for prescriptions written for URTIs. Indeed, the size of the reduction in overall prescribing was greater than anticipated from other studies, and suggests that there may have been an effect on reducing unnecessary prescribing for other indications. We did not attempt to ascertain whether there was a reduction in presentations with respiratory tract infections at the general practices. It is possible that such a reduction may have contributed to the fall in prescriptions, although state-wide epidemiological data on viral respiratory infections, which tend to drive antibiotic prescribing, show there were more influenza and other respiratory illnesses during the project year than the preproject year.23
There was an older age profile for the population within the study region compared with Australian population figures, and this might limit the generalisability of the findings. However, it might be argued that because the target population was local children and their parents, the potential to influence prescribing in other areas where there are higher percentages of children is even greater.
Finally, the study was not designed to measure the sustainability of the intervention. Short-term effects have been seen with a variety of interventions to reduce unnecessary prescribing for URTIs, but sustainable long-term reductions are being sought.24
In conclusion, we found that a community-based approach, involving GP education and the distribution of educational materials throughout the community was well received and successful in reducing dispensing of antibiotics for URTIs.
Based on the results of this project, the intervention has been rolled out across the state in conjunction with the Divisions of General Practice, the Department of Education and Children’s Services, and private schools, and an evaluation is planned for 2005 which will provide an opportunity to assess the sustainability of the program on the QUM Coast.
1 Clinical score to reduce unnecessary antibiotic use in patients with sore throat8
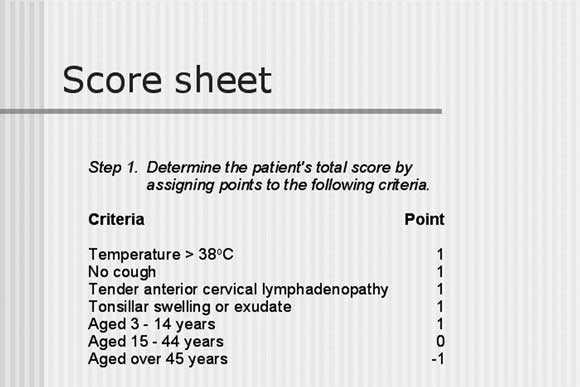 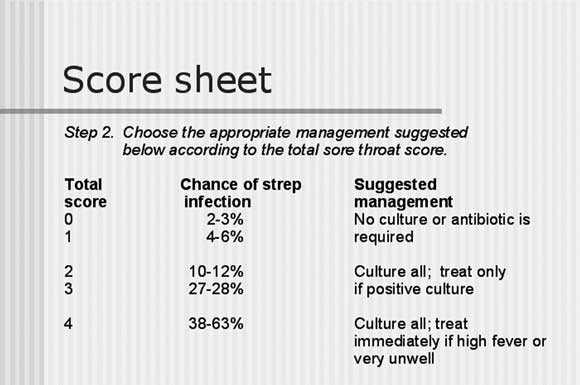 |
Reprinted from CMAJ 13 Jan 19988 by permission of the Canadian Medical Association.
2 Population demographic characteristics for age and sex19
Project region |
Australia |
||||||||||||||
Age (years) |
Male |
Female |
Total |
Male |
Female |
Total |
|||||||||
0–14 |
8.4% |
8.0% |
16.4% |
10.6% |
10.0% |
20.6% |
|||||||||
15–29 |
6.2% |
5.8% |
12.1% |
10.3% |
10.1% |
20.5% |
|||||||||
30–49 |
11.5% |
12.1% |
23.5% |
14.5% |
15.0% |
29.5% |
|||||||||
50–64 |
9.6% |
11.0% |
20.7% |
8.0% |
7.9% |
15.9% |
|||||||||
65+ |
12.5% |
14.4% |
26.9% |
5.5% |
7.0% |
12.5% |
|||||||||
Overseas visitors |
— |
— |
0.4% |
— |
— |
1.1% |
|||||||||
3 Dispensing volume of the six antibiotics most likely to be prescribed for upper respiratory tract infections for the preproject (1 June to 31 October 2000) and project (1 June to 31 October 2001) periods
|
Volume of drug dispensed (defined daily doses per 1000 population per day) |
|||||||||||||
Antibiotic |
Jun |
Jul |
Aug |
Sept |
Oct |
Total (Jun–Oct) |
Change |
|||||||
Amoxycillin |
||||||||||||||
Preproject |
2.2 |
2.9 |
3.4 |
3.5 |
2.9 |
14.8 |
+ 2.8% |
|||||||
Project |
2.6 |
2.7 |
3.1 |
3.6 |
3.3 |
15.2 |
|
|||||||
Amoxycillin/clavulanic acid |
||||||||||||||
Preproject |
2.1 |
2.6 |
3.1 |
3.4 |
2.0 |
13.2 |
− 8.1% |
|||||||
Project |
2.2 |
2.3 |
2.4 |
2.6 |
2.6 |
12.2 |
|
|||||||
Cefaclor |
|
|
|
|
|
|
|
|||||||
Preproject |
0.6 |
0.8 |
1.1 |
1.1 |
0.6 |
4.2 |
− 57.1% |
|||||||
Project |
0.5 |
0.3 |
0.3 |
0.4 |
0.3 |
1.8 |
|
|||||||
Doxycycline (all pack sizes) |
||||||||||||||
Preproject |
2.8 |
3.7 |
3.4 |
2.9 |
2.8 |
15.6 |
− 31.4% |
|||||||
Project |
2.2 |
2.4 |
2.3 |
2.2 |
1.7 |
10.7 |
|
|||||||
Erythromycin |
|
|
|
|
|
|
|
|||||||
Preproject |
1.4 |
2.5 |
2.7 |
2.1 |
1.5 |
10.2 |
− 69.6% |
|||||||
Project |
0.6 |
0.6 |
0.6 |
0.7 |
0.6 |
3.1 |
|
|||||||
Roxithromycin |
|
|
|
|
|
|
|
|||||||
Preproject |
3.1 |
4.5 |
3.8 |
4.4 |
3.0 |
18.7 |
− 30.8% |
|||||||
Project |
2.2 |
2.6 |
2.4 |
2.7 |
3.0 |
12.9 |
|
|||||||
Total antibiotics |
|
|
|
|
|
|
|
|||||||
Preproject |
12.5 |
16.6 |
17.5 |
17.3 |
12.9 |
77.1 |
− 31.5% |
|||||||
Project |
9.6 |
10.3 |
10.5 |
11.5 |
11.0 |
52.9 |
|
|||||||
Doxycycline (small pack sizes) |
||||||||||||||
Preproject |
1.5 |
1.5 |
1.4 |
1.2 |
1.1 |
6.8 |
− 49.1% |
|||||||
Project |
0.8 |
0.9 |
0.6 |
0.7 |
0.5 |
3.4 |
|
|||||||
Competing interests
None identified.
Acknowledgements
We gratefully acknowledge the Adelaide Southern Division of General Practice for their endorsement and support of the project; Ms Debra Kay, Manager Interagency Health Care, Department of Education and Children’s Services, for promoting the project to the schools within the project region; the QUM Coast Steering Committee, local general practitioners, pharmacists and other health care professionals, schools, childcare facilities and community groups for their support and enthusiasm in promoting and distributing the consumer information pamphlets. The South Australian Department of Health funded the intervention through the Quality Use of Medicines Program of the Drug Policies & Programs Branch, and were not involved in study design, conduct, interpretetation or publication.
References
- JETACAR: Joint Expert Advisory Committee on Antibiotic Resistance. The use of antibiotics in food-producing animals: antibiotic-resistant bacteria in animals and humans. Canberra: Commonwealth Department of Health and Aged Care and Commonwealth Department of Agriculture, Fisheries and Forestry 1999, [cited 2004 August 26]. Available at: http://www.health.gov.au/pubs/jetacar.pdf (accessed May 2005).
- Turnidge J. Responsible prescribing for upper respiratory tract infections. Drugs 2001; 61: 2065-2077. i1086465
- Bradley CP. Uncomfortable prescribing decisions: a critical incident study. BMJ 1992; 304: 294-296. i1086467
- McFarlane J, Holmes W, Macfarlane R, Britten N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: questionnaire study. BMJ 1997; 315: 1211-1214. i1086469
- Britten N, Ukoumunne O. The influence of patients’ hopes of receiving a prescription on doctors’ perceptions and the decision to prescribe: a questionnaire survey. BMJ 1997; 315: 1506-1510. i1086471
- De Santis G, Harvey KJ, Howard D, et al. Improving the quality of antibiotic prescription patterns in general practice. Med J Aust 1994; 160: 502-505. i1086473
- Molstad S, Ekedahl A, Hovelius B, Thimansson H. Antibiotics prescription in primary care: a 5-year follow-up of an educational programme. Fam Pract 1994; 11: 282-286. i1086475
- McIsaac W, White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ 1998; 158: 75-83. i1086477
- Cates C. An evidence based approach to reducing antibiotic use in children with acute otitis media. BMJ 1999; 318: 715-716. i1086479
- Bauchner H, Pelton SI, Klein JO. Parents, physicians, and antibiotic use. Pediatrics 1999; 103: 395-401. i1086481
- The National Strategy for Quality Use of Medicines. Canberra: Department of Communications, Information Technology and the Arts, 2002 [cited 2004 August 26]. Available at: http://www.nmp.health.gov.au/pdf/natstrateng.pdf (accessed May 2005).
- McIsaac WJ, Goel V, To T, Low DE. The validity of a sore throat score in family practice. CMAJ 2000; 163: 811-815. i1086485
- Dollman WB, LeBlanc VT, Stevens L, et al. Achieving a sustained reduction in benzodiazepine use through implementation of an area wide multi-strategic approach. J Clin Pharmacol Ther 2005. In press. i1086487
- Therapeutic guidelines: antibiotic. Version 11, 2000. Melbourne: Therapeutic Guidelines Ltd, 2000. i1086489
- Australian statistics on medicines 1999–2000. Canberra: Australian Government Department of Health and Ageing, 2003. Available at: http:// www.health.gov.au/internet/wcms/publishing.nsf/Content/health-pbs-general-pubs-asm.htm (accessed May 2005).
- Microsoft Access 97 [computer program]. US: Microsoft Corporation, 1997. i1086493
- SPSS Base 10.0 [computer program]. Chicago: SPSS Inc, 1999. i1086495
- Microsoft Excel 2000 [computer program]. US: Microsoft Corporation, 2000. i1086497
- Australian Bureau of Statistics. 2001 census: basic community profiles and snapshots. Available at: http://www.ausstats.abs.gov.au/ausstats/2001maps.nsf/0/7b31121743c8d5f6ca256bb90004a0b7?OpenDocument (accessed June 2005).
- Pharmaceutical benefits schedule item statistics. Canberra: Health Insurance Commission, 2003 [cited 2004 January 9]. Available at: http://www.hic.gov.au/statistics/dyn_pbs/forms/pbs_tab1.shtml (accessed May 2005).
- Bowman J, Kingsland M. NPS evaluation report no. 2. Sydney: National Prescribing Service, 2000. i1086503
- Wutzke S, Mandryk J, Harris G, et al. NPS evaluation report no. 5. Sydney: National Prescribing Service, 2002. i1086505
- Flu and respiratory illness charts. Adelaide: Communicable Disease Control Branch, 2002 [cited 2004 January 9]. Available at: http://www.dhs.sa.gov.au/pehs/notifiable-diseases-summary/resp_charts.htm (accessed May 2005).
- Welschen I, Kuyvenhoven MM, Hoes AW, Verheij TJM. Effectiveness of a multiple intervention to reduce antibiotic prescribing for respiratory tract symptoms in primary care: a randomised controlled trial. BMJ 2004; 329: 431. Epub 2004 Aug 05. i1086509