





Volume 182 - Issue 10
Tropical sprue in Far North Queensland
Author: Joshua P Hanson
Med J Aust 2005; 182 (10): 536-537. || doi: 10.5694/j.1326-5377.2005.tb00022.x
Published online: 16 May 2005
Published online: 16 May 2005
Clinical records
Patient 1
A 31-year-old Indigenous man from a remote Cape York community was referred for investigation of weight loss from 57 kg to 36 kg over the previous 3 years. He drank alcohol heavily and had had seizures which were probably related to this alcohol use. He had diffuse crusted scabies and there was obvious wasting.
His haemoglobin level was 90 g/L (normal range [NR], 130–180 g/L) with a mean cell volume (MCV) of 97 fL (NR, 80–100 fL). His white cell count was 11.4 × 109/L (NR, 4–11 × 109/L) with an eosinophilia of 4.34 × 109/L (NR, 0.04–0.4 × 109/L). The platelet count was normal. His ferritin level was 430 μg/L (NR, 30–300 μg/L) and levels of serum vitamin B12 and red cell folate were normal. The prothrombin time was 18 seconds (NR, 11–15 seconds). The albumin concentration was 16 g/L (NR, 35–45 g/L).
Upper abdominal ultrasound showed diffuse increased echogenicity of the liver. Stools had no white cells, red cells, bacterial pathogens, ova, cysts or parasites. Skin scrapings confirmed the clinical diagnosis of scabies.
Results of serological testing for HIV, strongyloides and coeliac disease were negative. He was deficient in vitamin A (0.1 μmol/L; NR, 1.6–2.3 μmol/L), 25-hydroxyvitamin D (< 12 nmol/L; NR, 25–150 nmol/L) and vitamin E (6 μmol/L; NR, 11–45 μmol/L).
Despite a high-protein and high-calorie diet, on Day 13 of his admission his weight was 34.4 kg. Small bowel biopsies taken at upper gastrointestinal endoscopy showed partial villous atrophy and a significant increase in inflammatory cells within the lamina propria. The endoscopic findings suggested tropical sprue, and prompted commencement of doxycycline and folate therapy. His weight improved immediately, and on discharge 10 days later he weighed 38.5 kg.
Ten weeks after discharge, despite continuing to misuse alcohol, he had gained 7.6 kg. His albumin level had increased to 33 g/L and the prothrombin time was 11 seconds. His haemoglobin level was 136 g/L, and white cell and eosinophil counts were normal.
Patient 2

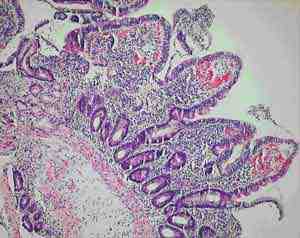
1 Upper gastrointestinal biopsy on Day 13 of admission
2 Upper gastrointestinal biopsy on Day 24 of doxycycline and folic acid therapy
A 62-year-old Indigenous man from a community near Cairns presented for investigation of weight loss, diarrhoea and macrocytic anaemia. He drank alcohol heavily and weighed only 39.5 kg.
Investigations showed a haemoglobin level of 73 g/L, MCV of 97 fL, a white cell count of 3.9 × 109/L and a platelet count of 97 × 109/L (NR, 150–400 × 109/L). The blood film showed hypersegmented neutrophils and macrocytes. His serum vitamin B12 level was normal and red cell folate level was < 73 nmol/L (NR, 295–1800 nmol/L). His ferritin level was 244 μg/L.
His potassium level was 2.3 mmol/L (NR, 3.4–4.5 mmol/L) and creatinine clearance was normal. His albumin level was 30 g/L, but other liver function test results were normal. Thyroid function was normal. Upper gastrointestinal endoscopy and biopsy performed on Day 13 of admission showed partial villous atrophy and increased inflammatory cells in the lamina propria (Figure 1).
Therapy with doxycycline and folic acid was begun on Day 17 of admission.
Follow-up endoscopy and biopsy 24 days after commencing this therapy showed a persistent inflammatory exudate, but an improvement in the villous appearance (Figure 2). By discharge, his haematological and biochemical test results were normal, his diarrhoea had stopped and his weight had improved to 47.3 kg.
Patient 3
A 66-year-old Indigenous man from a community near Cairns was referred for investigation of diarrhoea and weight loss. He had previously had a hemicolectomy for diverticular disease. He had lost 15 kg over 3 months and was having significant diarrhoea. In the week before referral he had shortness of breath on minimal exertion. On examination, he weighed 42 kg and was emaciated.
Investigations showed a haemoglobin level of 64 g/L with an MCV of 108 fL, a white cell count of 2.6 × 109/L and a platelet count of 40 × 109/L. A blood film showed hypersegmented neutrophils and macrocytes. His serum folate level was 3.2 nmol/L (NR, 6.6–35.3 nmol/L), vitamin B12 level was 137 pmol/L (NR, > 210 pmol/L) and ferritin level was 408 μg/L. The prothrombin time was 14 seconds.
His sodium level was 129 mmol/L (NR, 135–145 mmol/L), potassium level was 1.6 mmol/L, urea level was 8.2 mmol/L (NR, 2.5–8.0 mmol/L) and the creatinine level was 0.16 mmol/L (NR, 0.05–0.12 mmol/L). Liver function test results were otherwise normal.
Stool microscopy showed no white or red cells, ova, cysts or parasites, and no bacterial pathogens.
Upper gastrointestinal biopsy performed on Day 4 of admission showed atrophic villi and an inflammatory infiltrate in the lamina propria.
Vitamin B12 and folate supplementation were commenced on the day of admission and doxycycline therapy on Day 7. In the first week of antibiotic therapy, he gained 3 kg and his diarrhoea stopped. His white cell and platelet count became normal and haemoglobin level improved to 79 g/L. His biochemical test results normalised entirely. He was discharged home on Day 12 and booked for repeat endoscopy, but did not return.
The clinical presentation, histological findings and response to tetracycline and folate therapy in our patients, seen at Cairns Base Hospital between 1998 and 2004, support a diagnosis of tropical sprue. To our knowledge, these are the first reported cases in Australia.
All of our patients were Indigenous patients living in remote Indigenous communities. The alcohol use by the first patient clouds the picture, as high alcohol intake is associated with nutritional deficiencies. However, the partial villous atrophy on biopsy is more suggestive of tropical sprue. Additionally, despite being in hospital and not drinking alcohol for 2 weeks, there was no response in his weight or biochemical test results until therapy for tropical sprue commenced. Finally, his weight gain and improvement in biochemical test parameters continued despite ongoing alcohol misuse on discharge.
Seeing resolution of the histological changes in all the patients as they responded to treatment would have been desirable, but their remote location and the fact that two did not attend for follow-up made this difficult. It would also have been interesting to examine the small bowel flora of the patients, but this was not prospectively considered.
The absence of an agreed definition for tropical sprue has created difficulties. It has been noted that many asymptomatic people living in the tropics will have subclinical malabsorption and even abnormal small bowel biopsy results when rigorously assessed. Uncertainty in the diagnosis of tropical sprue is compounded by the condition’s incompletely understood aetiology. It is proposed that gastrointestinal infections, which occur at a higher rate in the tropics, cause mucosal injury and initiate the process. The mucosal injury leads to a disturbance in intestinal motility, allowing the overgrowth of coliform bacteria in the small bowel.1,2 Enterotoxins from these bacteria potentiate the mucosal damage which leads to malabsorption and protein loss. The resulting nutritional deficiencies hinder epithelial recovery, and a vicious circle develops. Alteration in the intestinal microflora may also lead to a change in toll-like receptor signalling and further retardation of intestinal healing.3
It seems likely that tropical sprue is not a single disease, but rather a pathophysiological process with heterogeneous manifestations resulting from subtle differences in the interplay of the initiating infection and the patient’s diet, living standards and genetics.4 A milder form of the process may lead to asymptomatic abnormalities — sometimes referred to as tropical enteropathy — while more severe expression may lead to the classical debilitating tropical sprue syndrome. The nature and the extent of the nutritional deficiencies are likely to be related to the duration of the disease and the extent of bowel involved.
Admission rates for gastroenteritis in Australia are nearly seven times higher in Indigenous communities than in non-Indigenous communities. Rates are also higher in regional and remote areas than in urban settings.5 Our own analysis of hospital separation data from Queensland’s northern zone for 1996–2001 shows an age-standardised hospital separation rate for gastrointestinal infection 2.32 times higher for Indigenous patients than non-Indigenous patients (95% CI, 2.17–2.48).
A number of studies of chronic diarrhoea in Indigenous Australian children have documented partial villous atrophy on small bowel biopsy.6,7 Higher colony counts and more frequent isolation of gram-negative organisms are found in duodenal aspirates from Indigenous children with chronic diarrhoea.8 Some of these studies noted a similarity with contemporary Indian studies of tropical sprue, but therapy with antibiotics and folate does not seem to have been considered in the Indigenous children.
Our anatomical pathology service believes that small-bowel biopsies from Indigenous patients from remote communities do show a subtle increase in inflammatory cells (Dr M Jagusch, Anatomical Pathology Department, Cairns Base Hospital, personal communication), perhaps representing the subclinical tropical enteropathy described above. The relatively high incidence of gastrointestinal infections in these Indigenous communities may explain these histological findings and, by initiating the pathological process, may predispose these populations to tropical sprue.
Dramatic presentations like those we describe are uncommon, but doctors working with remote Indigenous populations frequently encounter patients with evidence of milder nutritional deficiency. While there are many factors to consider in the assessment of poor nutrition in this population, and tropical sprue is a diagnosis of exclusion, the availability of a cheap, safe and rapidly effective treatment mandates that the diagnosis be considered in the appropriate clinical situation.
Lessons from practice
Tropical sprue should be considered in patients presenting with chronic weight loss, diarrhoea and nutritional deficiency.
While the aetiology of the disease is by no means clear, the high rates of gastrointestinal infection in remote Indigenous communities may predispose this group to the condition.
Tetracycline and folic acid therapy can be rapidly and dramatically effective, although the tetracycline course should continue for 3–6 months.
Competing interests
None identified.
Acknowledgements
I acknowledge the advice of Dr C Hadfield, Dr P Marshall, Dr C Boutlis and Professor M Gracey in preparing this manuscript. I also thank Brad McCulloch and Fiona Tulip at the Tropical Public Health Unit in Cairns for statistical analysis and advice.
References
- Cook GC. Aetiology and pathogenesis of post-infectious tropical malabsorption (tropical sprue). Lancet 1984; 1: 721-723.
- Glynn J. Tropical sprue — its aetiology and pathogenesis. J Roy Soc Med 1986; 79: 599-606. i1085779
- Rakoff-Nahoum S, Paglino J, Eslami-Varzaneh F, et al. Recognition of commensal microflora by toll-like receptors is required for intestinal homeostasis. Cell 2004; 118: 229-241. i1085781
- Menendez-Corrada R, Nettleship E, Santiago-Delphin EA. HLA and tropical sprue. Lancet 1986; 2: 1183-1185. i1085783
- Gracey M, Lee AH, Yau KK. Hospitalisation for gastroenteritis in Western Australia. Arch Dis Child 2004; 89: 768-772. i1085785
- Walker Smith JA, Reye RDK. Small intestinal morphology in Aboriginal children. Aust N Z J Med 1971; 4: 377-384. i1085787
- Harris MJ, Duffy BJ, Beveridge J. Studies on the bowel of a group of New South Wales Aboriginal children. Med J Aust 1970; 1: 356-359. i1085789
- Gracey M, Stone DE. Small intestinal microflora in Australian Aboriginal children with chronic diarrhoea. Aust N Z J Med 1972; 3: 215-219. i1085791