




Children's mental health forms an essential part of their overall health and wellbeing. According to recent epidemiological surveys, 11%–15% of Australian children (aged 13 years and younger) and 13%–17% of young people (14–18 years old) experience significant mental health problems, conduct problems, depression, and anxiety.1-3 This rate increases to 25%–35% in early adulthood.4 The National Action Plan for the Promotion, Prevention and Early Intervention for Mental Health5 argues for the importance of evidence-based early intervention programs by national, State and Territory governments to prevent serious childhood behaviour problems.6,7
Any serious attempt to improve the mental health of children needs to address the quality of parenting that children receive as well as the quality of their family relationships. There is substantial evidence linking parenting and family risk factors to the development of serious conduct problems in children. These include the lack of a warm, positive relationship with parents; insecure attachment; harsh, inflexible, rigid, or inconsistent discipline practices; inadequate supervision of, and involvement with, children; marital conflict and breakdown; and parental psychopathology (particularly maternal depression and high levels of parenting stress). These factors increase the risk of children developing major behavioural and emotional problems, including conduct problems, substance misuse, antisocial behaviour, and participation in delinquent activities.8-10 Additionally, for many children, there is increasing evidence of a link between internalising disorders (such as anxiety and depression) and externalising disorders (such as disruptive behaviour disorders).11 Specifically, when children develop conduct problems in association with internalising disorders, their risk of developing significant depression and anxiety in adolescence and young adulthood is increased.
Other evidence for a link between family factors and depression and anxiety comes from the child abuse literature. Higher levels of depression, conduct disorder, social deficits, and other internalising and externalising disorders occur in adolescents who have been physically abused as young children.12,13 A wide range of serious adolescent risk behaviours is associated with abuse, including early sexual activity, pregnancy, eating disorders, emotional disorders (such as depression and anxiety), suicide attempts, and drug and alcohol misuse. Parents of children with, or who are at risk of, developing emotional or behavioural problems are often less confident in their parenting role; find parenting to be stressful, demanding and depressing; and experience more conflict with relationship partners over parenting issues.14
Although there are well-developed parenting and family-based interventions that are effective in treating many common childhood behaviour problems, these interventions are not widely available in the community, and therefore have a negligible effect on the prevalence of children's behaviour difficulties. Here, I examine the role of a population strategy that incorporates the media and professionals in primary care services (ie, general practitioners, child health nurses, teachers, childcare workers, and allied health professionals) as part of a comprehensive parenting and family support system to improve the health status and wellbeing of children.
Of the interventions that target parenting and family relationships, behavioural family interventions (BFI) based on social learning models have the strongest empirical support and warrant serious consideration for broader population-level application.10 BFI are the most thoroughly evaluated interventions available to assist children with conduct problems.15-19 Typically, parents are taught to increase positive interactions with children and to reduce coercive and inconsistent parenting practices. BFI produce positive changes in parental perceptions and parenting behaviours, which in turn are associated with changes in child behaviours.20,21
The empirical basis of BFI is strengthened by evidence that the approach can be successfully applied to many other clinical problems and disorders, including attention-deficit hyperactivity disorder,22 persistent feeding difficulties,23 recurrent pain syndromes,24 anxiety disorders,25 autism and developmental disabilities,26 achievement problems, habit disorders, and common childhood problems (for reviews, see references 18 and 19). Parenting and family-oriented interventions have also been increasingly used with parents of adolescents at risk of drug use, conduct problems and delinquency, attention-deficit disorder, eating disorders, depression, and chronic illness.27,28
Meta-analyses of treatment-outcome studies of BFI often report large effect sizes29 with good maintenance of treatment gains.30 For instance, treatment effects for children have been shown to generalise to school settings31 and to various community settings outside the home.32 Parents participating in these programs are generally satisfied consumers.33 Additionally, BFI reduce maternal depression and stress, increase parental satisfaction and efficacy, and reduce marital conflict over parenting issues.34-37 Various different delivery formats are effective, including individually administered face-to-face programs,38 group programs,39 telephone-assisted programs,40 and self-directed programs.41 The success of BFI highlights the importance of including parenting interventions in any comprehensive preventive intervention designed to reduce behavioural and emotional problems in children.
For an intervention to be considered suitable for implementation at a population level, several conditions need to be met. It has been argued that these conditions include having:
evidence available about the prevalence of the target problem (child behavioural and emotional problems) and associated risk factors to be targeted (parenting variables);
evidence which shows that modifying the risk factor is associated with improvements in the targeted problem;
an effective, culturally appropriate intervention available that can be readily disseminated; and
a delivery mechanism to enable the program to be widely implemented in the community.35
Within the Australian context, each of these conditions has been met sufficiently to warrant serious consideration for adopting a population-level approach.
Approaches to prevention are typically conceptualised as falling into one of three categories: universal, selective, or indicated.42 A universal prevention strategy targets an entire population (eg, national, local community, neighbourhood, school). Selective prevention programs target specific subgroups of the general population (eg, low-income families, young single mothers) that are believed to be at greater risk than others for developing a problem. Indicated preventive interventions target high-risk individuals who are identified as having detectable problems (eg, disruptive and aggressive children) but who do not yet meet diagnostic criteria for a behavioural disorder.
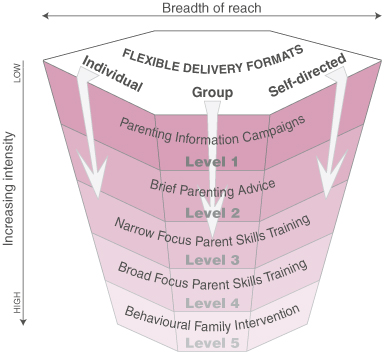
Triple P is a multilevel parenting and family support strategy I developed with my colleagues at the University of Queensland.43 The program aims to prevent severe behavioural, emotional and developmental problems in children by enhancing the knowledge, skills and confidence of parents. It incorporates universal, selective and indicated interventions organised across five levels on a tiered continuum of increasing strength (see Box 1).
Triple P has been implemented in a range of health, education and welfare settings throughout Australia. Triple P training courses have been conducted in all Australian States and Territories, except Tasmania and the Australian Capital Territory, and there is a growing number of accredited providers in Australia, New Zealand, the United Kingdom, the United States, Germany, Switzerland, Hong Kong, and Singapore. The program has been successfully trialled in a range of diverse cultural contexts, including Chinese and Vietnamese, Arabic, Maori, and Pacific Islander groups, and is currently being evaluated with Indigenous parents in Queensland. Limited program resources and materials have been translated into several other languages. Several derivative programs have been developed and trialled. These include Stepping Stones Triple P, a version of the program for parents of children with disabilities, and Pathways Triple P, a version targeting parents involved in the child protection system.
Triple P addresses the broader context by making parenting strategies available to all parents in the community. When fully implemented, the system is a coordinated set of multilevel strategies to provide parents with easy access to information and support about effective parenting. It offers a tiered continuum of interventions of increasing intensity (Levels 1–5; see Box 1 and Box 2), and a specialised intervention for indicated families at highest risk for continued or future child maltreatment. By matching the level of intensity to family need, making parenting information and support broadly accessible to all parents, and promoting the same overarching principles and strategies of positive parenting across all levels of intervention, the system aims to reduce stigma, normalise participation, build continuity across levels of intervention, and optimise population exposure.
The distinguishing features of the program include:
its universality;
the use of multiple levels of intervention to facilitate matching the intensity of intervention to the needs of each individual family;
its multidisciplinary nature;
the use of flexible delivery modalities (group, individual, self-directed, telephone-assisted); and
the program's aim of destigmatising access points (by use of primary healthcare services, schools, and childcare centres).
Its use of the mass media involves wide exposure and easy access to the program.
The universal parent information strategy (Level 1 of Triple P) provides all interested parents with access to useful information about parenting through a coordinated media and promotional campaign using print and electronic mass media, user-friendly parenting tip sheets, and videotapes that demonstrate specific parenting strategies. This level of intervention aims to increase community awareness of parenting resources, promote parents' receptivity to participate in programs, and create a sense of optimism by depicting solutions to common behavioural and developmental concerns. Level 2 is a brief, one- to two-session primary care selective intervention providing anticipatory developmental guidance to parents of children with mild behavioural difficulties. Level 3, a more intensive four-session selective intervention, is designed for parents of children with mild to moderate behavioural difficulties, and includes active skills training for parents. Level 4 is an intensive eight- to 10-session individual or group training program for parents of children with more severe behavioural difficulties. Level 5 is a five- to 11-session enhanced BFI program for families with parenting difficulties complicated by other sources of family distress (eg, relationship conflict, parental depression, or high levels of stress). It builds on Level 4, with additional modules targeting home practice of parenting skills, coping skills, and partner support skills.
This tiered multilevel strategy recognises that there are differing levels of dysfunction and behavioural disturbance in children and adolescents, and that parents have differing needs and desires regarding the type, intensity and mode of assistance they require. The system is designed to maximise efficiency, contain costs, avoid waste and overservicing, and ensure that the program has wide reach in the community. The program targets five different developmental periods, from infancy to adolescence, and within each developmental period the reach of the intervention can vary from broad (targeting an entire population) to narrow (targeting only high-risk children). The multidisciplinary nature of the program involves the better utilisation of the existing professional workforce in promoting competent parenting. The design of the program enables considerable flexibility for the practitioner in tailoring the program to the specific needs of families.
A large number of paediatric consultations deal with parental concerns about a child's behaviour, development, or school achievement.19,44-47 The past decade has seen an increasing emphasis on treating mental health problems at the primary care level.48 A recent parenting survey showed that family doctors are the professionals most frequently consulted by caregivers of children with an emotional or behavioural problem.49 Similarly, the Western Australian Child Health Survey showed that 65% of parents of children with behavioural and emotional problems consulted a doctor during a six-month period, yet only 2% saw a mental health specialist.2 Although primary care professionals are well positioned to provide parenting support, they are commonly under-resourced and undertrained for detecting child behavioural problems and providing effective mental health programs for children and families.
In reporting a US national survey of more than 2000 parents with children under three years of age, Young and colleagues highlighted parents' concerns and the information they would like to receive from their paediatric physician or nurse.50 Most parents reported having a regular source of paediatric healthcare which met their child's health needs, yet many were not satisfied with the help they received with regard to understanding their child's growth, development, or care. Less than a quarter had talked with their paediatric clinician about discipline or promoting their child's development. Parents who received this type of information were significantly more satisfied with their paediatric clinician than those who had not. Most parents (79%) reported a desire for more information from their paediatric clinician in at least one of six areas of childrearing (newborn care, sleep patterns, crying, toilet training, discipline, encouraging early learning). These data suggest that personalised advice, in the context of an ongoing supportive relationship, is the need being expressed by parents.
As primary care services have regular contact with young families, they can undertake several important tasks to promote children's mental health. Early detection of significant deviations from normal development and provision of advice to parents seeking information about developmental issues can become part of routine well-child care. Provision of brief behavioural counselling for child behavioural problems and increased access to early intervention for dysfunctional family interaction patterns could help prevent later, more serious problems.
Primary care service providers can be supported to perform a triage function for the appropriate referral of children with moderate to severe behaviour problems to specialised services, and be better informed about available mental health services in the community. This helps match intervention strength to individual family needs and ensures that the funds available for specialist mental health services are directed where they are most needed. In the long term, widespread implementation of preventive primary care interventions could decrease the number of children requiring specialist mental health services. Through this type of primary care strategy, parent education and support in preventing and managing childhood emotional and behavioural problems becomes an integral part of family healthcare provision.
The evidence base documenting the efficacy of Triple P is extensive. Several published randomised controlled trials examined the effect of different levels of the intervention and delivery modalities.35,36 Typically, parents receiving Triple P interventions report that their children are less disruptive and more cooperative. These reports of positive behaviour changes have been verified by independent behavioural observations in the home. Parents also report higher levels of self-efficacy in their parenting role, less coercive discipline, less depression and stress, and lower levels of marital conflict over parenting. Moderate to large effect sizes are typically reported with high levels of consumer satisfaction (for a review of the evidence base, see reference 43). In addition to this work, several trials documenting the efficacy of Triple P as a primary care intervention have been completed, and at time of writing are under review or are in the process of submission.
Collective results from these trials provide a strong basis for the use of Triple P as an early intervention strategy to manage child problem behaviours in primary care.
That only a small proportion of children with significant mental health problems have contact with mental health services2 indicates there are significant barriers to service utilisation. Several steps can be undertaken to improve community awareness of parenting issues and enhance service provision. Greater community education through the mass media regarding parenting issues can directly influence parenting practices and may optimise early help-seeking.51 To improve detection rates, optimal training for primary care professionals should focus on increasing awareness of the nature and prevalence of mental health problems in their patients, and the characteristics of high-risk groups.48,51 Training primary care practitioners in brief prevention and early intervention programs, and establishing appropriate referral and liaison mechanisms with specialist mental health services,52-54 would help to ensure optimal care for patients presenting with mental health, behavioural or social concerns. Triple P training for GPs has been successfully trialled in Queensland, with more than 350 GPs participating in a two-day training course organised through the Queensland Divisions of General Practice.
Primary care services are well placed to offer parenting support in the community through early detection of problems, provision of advice to parents about developmental issues, provision of empirically supported prevention and early intervention programs for mild to moderate child behaviour problems, and appropriate referral to specialist services for moderate to severe problems. As most paediatric clinicians do not feel adequately prepared to provide such a service,46,50 primary care professionals need better training and access to high quality, well-researched information resources to use in consultations with parents about developmental and behavioural issues.19
Commonly expressed concerns are that the provision of training to primary healthcare practitioners to deliver parent training will reduce the role of specialist mental health practitioners, and that families will be harder to work with if there have been unsuccessful, less intensive interventions. Our experience has been rather different. With relevant training, primary care practitioners develop knowledge of the type and intensity of intervention needed, and are more inclined to implement early interventions and make appropriate referrals to other professionals. If primary care professionals develop better detection strategies and are more aware of local services, it is likely that mental health services will be better accessed by families in need of specialist services, while less severe cases are dealt with in self-directed and primary care prevention programs. An examination of the number and nature of referrals from primary care settings may clarify this issue.
Interventions that provide more predictable, stable, nurturing, responsive and contingent parenting will reduce family risk factors associated with the development of depression, anxiety and serious conduct problems in children. There is now sufficient evidence for governments to seriously consider funding the broad implementation of well-established, empirically supported parenting and behavioural family intervention programs to improve the mental health status of children. Effective prevention strategies must address parenting practices and family relationships. A multilevel approach that involves a tiered continuum of increasingly intensive family interventions using a population health approach is required. Further research is being undertaken by our research group to examine which families respond to which levels of intervention, particularly to determine the type of support primary care providers can offer to families at risk.
1: The Triple P model of parenting and family support
Level of intervention |
Target population |
Intervention methods |
Possible target areas |
||||||||
1. Universal Triple P |
|||||||||||
Media-based parenting information campaigns |
All parents interested in information about parenting and promoting their child's development. |
A coordinated information campaign using print and electronic media and other health promotion strategies to promote awareness of parenting issues and normalise participation in parenting programs such as Triple P. May include some contact with professional staff (eg, telephone information line). |
General parenting issues. Common everyday behavioural and developmental issues. |
||||||||
2. Selected Triple P |
|||||||||||
Information and advice for a specific parenting concern |
Parents with specific concerns about their child's behaviour or development. |
Provision of specific advice on how to solve common child developmental issues and minor child behavioural problems. May involve face-to-face or telephone contact with a practitioner (about 20 min over two sessions) or (60–90 min) seminars. |
Common behavioural difficulties or developmental transitions, such as toilet training, bedtime problems. |
||||||||
3. Primary Care Triple P |
|||||||||||
Narrow-focus parent skills training |
Parents with specific concerns about their child's behaviour or development who require consultations or active skills training. |
A brief program (about 80 min over four sessions) combining advice with rehearsal and self-evaluation as required, to teach parents to manage a discrete child problem behaviour. May involve face-to-face or telephone contact with a practitioner. |
Discrete child behavioural problems, such as tantrums, whining, fighting with siblings. |
||||||||
4. Standard Triple P/Group Triple P/Self-Directed Triple P |
|||||||||||
Broad-focus parent skills training |
Parents wanting intensive training in positive parenting skills. Typically targets parents of children with more severe behavioural problems. |
A broad-focus program (up to 12 one-hour sessions) for parents requiring intensive training in positive parenting skills and strategies designed to enhance the generalisation of these skills to different settings. Application of parenting skills to a broad range of target behaviours, settings and children. Program variants include individual, group, or self-directed (with or without telephone assistance) options. |
Multiple child behavioural problems. Aggressive behaviour. Oppositional defiant disorder. Conduct disorder. Learning difficulties. |
||||||||
5. Enhanced Triple P |
|||||||||||
Behavioural family intervention |
Parents of children with concurrent child behavioural problems and family dysfunction. |
An intensive, individually tailored program (up to 11 one-hour sessions) for families with child behavioural problems and family dysfunction. Program modules include home visits to enhance parenting skills, mood management strategies and stress coping skills, and partner support skills. |
Concurrent child behavioural problems and parent problems (eg, relationship conflict, depression, stress). |
||||||||
- Matthew R Sanders1
- School of Psychology, University of Queensland, Brisbane, QLD.
Preparation of this article was supported by a grant to the Parenting and Family Support Centre from Queensland Health.
The author is the Director of the Parenting and Family Support Centre, University of Queensland, which developed the Triple P – Positive Parenting Program.
- 1. Sawyer MG, Arney F, Baghurst P, et al. The mental health of young people in Australia. Canberra: Mental Health and Special Programs Branch, Commonwealth Department of Health and Aged Care, 2000. Available at <http://www.health.gov.au/hsdd/mentalhe/resources/young/pdf/young.pdf>.
- 2. Zubrick S, Silburn S, Garton A, et al. Western Australian child health survey: developing health and well-being in the nineties. Perth: Institute for Child Health Research and Australian Bureau of Statistics, 1995.
- 3. Zubrick S, Silburn S, Teoh H, et al. Western Australian child health survey: education, health and competence. Perth: Australian Bureau of Statistics and TVW Telethon Institute for Child Health Research, 1997.
- 4. Australian Bureau of Statistics. Mental health and wellbeing: profile of adults, Australia, 1997. Canberra: ABS, 1998. (Catalogue no. 4326.0.)
- 5. Commonwealth Department of Health and Aged Care. Promotion, prevention and early intervention for mental health: a monograph, 2000. Canberra: Mental Health and Special Programs Branch, Commonwealth Department of Health and Aged Care, 2000. Available at <http://www.health.gov.au/hsdd/mentalhe/mhinfo/ppei/pdf/monograph.pdf>.
- 6. Marshall J, Watt P. Child behaviour problems: a literature review of the size and nature of the problem and prevention interventions in childhood. Perth: Interagency Committee on Children's Futures, 1999.
- 7. National Crime Prevention. Pathways to prevention: developmental and early intervention approaches to crime in Australia. Canberra: National Crime Prevention, Attorney-General's Department, 1999. Available at <http://www.crimeprevention.gov.au/ncp/Publications/PDF/no6_fullreport.pdf>.
- 8. Coie, JD. Prevention of violence and antisocial behaviour. In: Peters RD, McMahon RJ, editors. Preventing childhood disorders, substance abuse, and delinquency. Thousand Oaks, CA: Sage Publications, 1996.
- 9. Loeber R, Farrington DP. Never too early, never too late: risk factors and successful interventions for serious and violent juvenile offenders. Stud Crime Crime Prev 1998; 7: 7-30.
- 10. Patterson GR. Coercive family process. In: Patterson GR, Reid JB, editors. A social learning approach to family intervention. Vol 3. Eugene, Oregon: Castalia Publishing, 1982.
- 11. Han S, Weiss B, Weisz R. Specificity of relations between children's control-related beliefs and internalising and externalising psychopathology. J Consult Clin Psychol 2001; 62: 240-251.
- 12. Horowitz K, Weine S, Jekel J. PTSD symptoms in urban adolescent girls: compounded community trauma. J Am Acad Child Adolesc Psychiatry 1995; 35: 1353-1361.
- 13. Pelcovitz D, Kaplan S, Goldenberg B, et al. Posttraumatic stress disorder in physically abused adolescents. J Am Acad Child Adolesc Psychiatry 1994; 33: 305-312.
- 14. Sanders M, Tully L, Baade P, et al. A survey of parenting practices in Queensland: implications for mental health promotion. Health Promot J Aust 1999; 9: 105-114.
- 15. Brestan EV, Eyberg SM. Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5,272 kids. J Clin Child Psych 1998; 27: 180-189.
- 16. Lochman JE. Modification of childhood aggression. In: Hersen M, Eisler RM, Miller PM, editors. Progress in behavior modification. Vol 25. Thousand Oaks, CA: Sage Publications, 1990; 47-85.
- 17. McMahon RJ. Parent training. In: Russ SW, Ollendick TH, editors. Handbook of psychotherapies with children and families. New York: Plenum Publishers, 2000.
- 18. Sanders M. New directions in behavioural family intervention with children. In: Ollendick T, Prinz R, editors. Advances in clinical child psychology. New York: Plenum Press, 1996; 283-330.
- 19. Taylor TK, Biglan A. Behavioral family interventions for improving child-rearing: a review of the literature for clinicians and policy makers. Clin Child Fam Psychol Rev 1998; 1: 41-60.
- 20. Barlow J, Stewart-Brown S. Behavior problems and group-based parent education programs. J Dev Behav Pediatr 2000; 21: 356-370.
- 21. Webster-Stratton C, Taylor TK. Adopting and implementing empirically supported interventions: a recipe for success. In: Buchanan A, Hudson BL, editors. Parenting, schooling and children's behaviour. Aldershot, UK: Ashgate, 1998; 127-160.
- 22. Barkley RA, Guevremont DC, Anastopoulos AD, Fletcher KE. A comparison of three family therapy programs for treating family conflicts in adolescents with attention-deficit hyperactivity disorder. J Consult Clin Psychol 1992; 60: 450-462.
- 23. Turner KMT, Sanders MR, Wall CR. Behavioural parent training versus dietary education in the treatment of children with persistent feeding difficulties. Behav Change 1994; 11: 242-258.
- 24. Sanders MR, Shepherd RW, Cleghorn G, Woolford H. The treatment of recurrent abdominal pain in children: a controlled comparison of cognitive-behavioral family intervention and standard pediatric care. J Consult Clin Psychol 1994; 62: 306-314.
- 25. Barrett PM, Dadds MR, Rapee RM. Family treatment of childhood anxiety: a controlled trial. J Consult Clin Psychol 1996; 64: 333-342.
- 26. Schreibman L, Kaneko WM, Koegel RL. Positive affect of parents of autistic children: a comparison across two teaching techniques. Behav Ther 1991; 22: 479-490.
- 27. Dishion TJ, Andrews DW. Preventing escalation in problem behaviors with high-risk young adolescents: immediate and 1-year outcomes. J Consult Clin Psychol 1995; 63: 538-548.
- 28. Irvine AB, Biglan A, Smolkowski K, et al. The effectiveness of a parenting skills program for parents of middle school students in small communities. J Consult Clin Psychol 1999; 67: 811-825.
- 29. Serketich WJ, Dumas JE. The effectiveness of behavioral parent training to modify antisocial behavior in children: a meta-analysis. Behav Ther 1996; 27: 171-186.
- 30. Forehand R, Long N. Outpatient treatment of the acting out child: procedures, long term follow-up data, and clinical problems. Adv Behav Res Ther 1988; 10: 129-177.
- 31. McNeil CB, Eyberg S, Eisenstadt TH, et al. Parent child interaction therapy with behaviour problem children: generalization of treatment effects to the school setting. J Clin Child Psychol 1991; 20: 140-151.
- 32. Sanders MR, Glynn T. Training parents in behavioural self-management: an analysis of generalization and maintenance. J Appl Behav Anal 1981; 14: 223-237.
- 33. Webster-Stratton C. Systematic comparison of consumer satisfaction of three cost-effective parent training programs for conduct problem children. Behav Ther 1989; 20: 103-115.
- 34. Nicholson JM, Sanders MR. Randomized controlled trial of behavioral family intervention for the treatment of child behavior problems in stepfamilies. J Divorce Remarriage 1999; 30: 1-23.
- 35. Sanders MR, Markie-Dadds C, Tully LA, Bor W. The Triple P-positive parenting program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. J Consult Clin Psychol 2000; 68: 624-640.
- 36. Sanders MR, McFarland M. Treatment of depressed mothers with disruptive children: a controlled evaluation of cognitive behavioral family intervention. Behav Ther 2000; 31: 89-112.
- 37. Webster-Stratton C. Preventing conduct problems in Head Start children: strengthening parenting competencies. J Consult Clin Psychol 1998; 66: 715-730.
- 38. Forehand RL, McMahon RJ. Helping the noncompliant child: a clinician's guide to parent training. New York: Guilford Press, 1981.
- 39. Webster-Stratton C. Systematic comparison of consumer satisfaction in three cost-effective parent training programs for conduct problem children. Behav Ther 1989; 20: 103-115.
- 40. Connell S, Sanders MR, Markie-Dadds C. Self-directed behavioral family intervention for parents of oppositional children in rural and remote areas. Behav Mod 1997; 21: 379-408.
- 41. Markie-Dadds C, Sanders MR. Self-directed Triple P-Positive Parenting Program for parents of children at high or low risk of developing conduct problems. In press, 2002.
- 42. Mrazek PJ, Haggerty RJ, editors. Reducing risks for mental disorders: frontiers for preventive intervention research. Washington, DC: National Academy Press, 1994.
- 43. Sanders MR. Triple P-Positive parenting program: towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clin Child Fam Psychol Rev 1999; 2: 71-90.
- 44. Christophersen ER. Incorporating behavioral pediatrics into primary care. Pediatr Clin North Am 1982; 29: 261-296.
- 45. Christophersen E. Behavioral pediatrics: an overview. In: McGrath PJ, Firestone P, editors. Pediatric and adolescent behavioral medicine: issues in treatment. New York: Springer, 1983; 1-12.
- 46. Oberklaid F, Dworkin PH, Levine MD. Developmental–behavioral dysfunction in preschool children. Descriptive analysis of a pediatric consultative model. Am J Dis Child 1979; 133: 1126-1131.
- 47. Triggs EG, Perrin EC. Listening carefully. Improving communication about behavior and development. Recognizing parental concerns. Clin Pediatr 1989; 28: 185-192.
- 48. Giel R, Koeter M, Ormel J. Detection and referral of primary-care patients with mental health problems: the second and third filter. In: Goldberg D, Tantam D, editors. The public health impact of mental disorder. Toronto: Hogrefe and Huber, 1990; 25-34.
- 49. Sanders M, Tully L, Baade P, et al. A survey of parenting practices in Queensland: implications for mental health promotion. Health Promot J Aust 1999; 9: 112-121.
- 50. Young KT, Davis K, Schoen C, Parker S. Listening to parents. A national survey of parents with young children. Arch Pediatr Adolesc Med 1998; 152: 255-262.
- 51. Vasquez-Barquero J. Mental health in primary care settings. In: Goldberg D, Tantam D, editors. The public health impact of mental disorder. Toronto: Hogrefe and Huber, 1990; 35-44.
- 52. Cotton P. Psychological services in primary care settings. Clin Psychol 1998; 3: 20-22.
- 53. Kramer M, Simonsick E, Lima B, Levav I. The epidemiological basis for mental health care in primary health care: a case for action. In: Cooper B, Eastwood R, editors. Primary health care and psychiatric epidemiology. London: Routledge, 1992; 69-98.
- 54. Nicholson J, French M, Oldenberg B, Connelly L. Evaluation of the mental health service in rural and remote South West Queensland: final report for the Southern Queensland Rural Division of General Practice. Brisbane: School of Public Health, Queensland University of Technology, 1997.
Abstract
The reduction of coercive or inadequate parenting is essential if the mental health status of Australian children and adolescents is to be improved.
Of the available approaches that address parenting practices, behavioural family interventions have the strongest empirical support and are effective in reducing parenting practices that contribute to the development of behavioural and emotional problems in children. However, only a small proportion of parents access such interventions.
A comprehensive multilevel, evidence-based parenting and family support strategy needs to be implemented on a wide scale to reduce the prevalence of mental health problems in children and youth.
The Triple P – Positive Parenting Program is an example of a population-level strategy that can be used to improve the mental health status of children and their parents.