




The Nobel laureate Max Perutz said it as well as anyone, "Making a discovery is such a wonderful thing. It's like falling in love and getting to the top of a mountain all in one."1 For those with a less romantic inclination, the words of Franklin D Roosevelt, 32nd President of the United States, might be more felicitous. He said, "We cannot be a strong nation unless we are a healthy nation".2
Those who have grown up as medical scientists feel most comfortable talking about the medical contributions of research:
the basic scientific discoveries in genetics, cell and molecular biology, neuroscience, and immunology;
the organ systems that we've explored using physiological, pharmacological, and imaging technologies;
the patients we've studied and the volunteers who have stepped forward to help us do clinical trials;
the medicines that have been discovered and developed by multidisciplinary teams in industry; or
the infectious diseases whose death tolls have been so dramatically reduced in the 20th century. The dramatic reductions in deaths due to influenza, tuberculosis, syphilis, diphtheria, pertussis, measles, poliomyelitis and smallpox rank as crowning achievements of medical research and public health.
Finally, it is important that we not forget that life expectancy in the United States has increased by more than five years in the past 30 years,3 a remarkable 7% increase that cannot be attributed to improvements in sanitation and public health measures, which increased longevity so much during the first two-thirds of the 20th century. These recent gains in life expectancy are a direct result of investments in medical research.
To me there is another treasured aspect of the field. That is, its global nature. Medical research is carried out by people in many countries for people in all countries. Australia has a rich heritage in medical research, as do many other developed countries. I am familiar with your "heroes" — Florey, Burnet, Eccles, Doherty, Metcalfe, and Marshall — just as you are with mine. However vigorously scientists around the world compete — and we do compete vigorously — we applaud the accomplishments of those who reach the summit of Perutz's metaphoric mountain, as well as the vast majority who don't get quite that high.
But I'm going to leave my comfort zone and address something else that is equally important to the future of medical research. Not genomics or proteomics; not reproductive or research cloning; and not bioethics and the protection of human subjects. I'm going to talk about money — money as it pertains to medical research. I will approach this by examining four avenues: the US financial investment in medical research; some estimates of the economic return on this investment; extrapolation of these findings to Australia; and consideration of the global implications of medical research.
I start with the United States, because the economic issues concerning medical research have been most elaborated and studied there. It might come as a surprise to some that the US government's commitment to medical research is only a recent event. Before World War II, industry and philanthropy invested more than 90% of whatever paltry sums went to support research.4 The government was essentially a non-player.
Some major American figures lamented this situation. Just before the Great Depression of 1929, President Herbert Hoover remarked that "some scientific discoveries and inventions have, in the past, been the result of genius struggling in poverty. But poverty does not clarify thought, nor furnish laboratory equipment."5 Albert Szent-Györgyi, the 1937 Nobel laureate for the discovery of vitamin C, observed, "Research is four things: brains with which to think, eyes with which to see, machines with which to measure and, fourth, money."6
Financial support for research in the US improved in the 1950s, thanks to the relocation to Bethesda of the National Institutes of Health (NIH), the advocacy of a few members of Congress such as Joseph Ransdell, Lister Hill, and James Fogarty and the lobbying efforts of Mary Lasker, the first Citizen Advocate for Medical Research, who stalked the halls of Congress urging greater appropriations for the NIH by saying things like, "If you think research is expensive, try disease".
The past 40 years have witnessed an impressive escalation of the US national investment in medical research. These increases occurred first in the expenditure of public funds through the NIH and, to a much lesser extent, other federal agencies. As basic science burgeoned in academia as a result of the enormous infusion of government grants, discoveries there were translated into new commitments and investments in research and development by the pharmaceutical industry, and into the birth and growth of the biotechnology industry. This pattern has continued to the present. The US federal government still sponsors the vast majority of medical research in academia. Industry still invests a significant fraction of its profits toward the discovery and development of new medicines, devices and diagnostic tests.
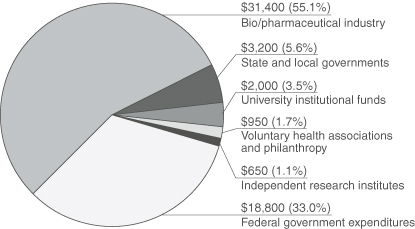
In 1999, the last year for which there are complete data, total US investments in medical and health research were about US$57 billion, or about US$250 per capita7 (Box 1). Sponsorship for this research came from six sources:
the federal government;
the biopharmaceutical industry;
state and local governments;
university funds;
voluntary health associations and philanthropy; and
independent research institutes (such as the Howard Hughes Medical Institute).
Industry is the largest financial sponsor, investing some US$31 billion, or 55% of the total US investment in medical research. The federal government's contribution (US$18.8 billion) is 33% of the total. It is important to point out that the other sponsors, even though proportionally much smaller, provide a total of US$7 billion and add a degree of flexibility and synergy to the national investment far beyond the dollar value.
In 1998, advocates led by Research!America, the Committee for Medical Research, and the Federation of American Societies for Experimental Biology called for a doubling of the NIH budget by 2003 — from US$13 billion to US$27 billion — believing that there were a great number of opportunities that weren't being taken up. Remarkably, this is coming to pass, thanks to annual increases in each of the past four years of nearly 15% voted by Congress and approved by Presidents Clinton and Bush.
What is less appreciated is that industry funding has grown even more. In 1999, the federal government's investment was about 59% of that in industry; this year that figure is about 55%. Once again, as government has primed the scientific pump, industry has responded, using the information gained to further the discovery and development of medicines and devices.
While some people claim that the United States spends a great deal on medical research — perhaps too much — I say we don't spend enough — only about five cents of the health dollar. Moreover, the public funding of medical research is only about two cents of the health dollar. I believe this amount should be increased, but many people in positions of power are sceptical. Increasingly, there are questions about the return on this investment. What is the public gaining for this financial support? These questions are being asked regularly by Congress and private investors.
There are many ways to estimate the economic return on medical research investments, such as the number of jobs created in the private sector, healthcare costs saved, the value of increased longevity, the value of reduced morbidity and disability, and the benefits of newer medicines. I will concentrate on the first three.
Job creation in the private sector is the easiest parameter to gauge. It is estimated that there are more than 500 000 people employed in the US biopharmaceutical industry in our country because of commitments to research and development.8,9 These high-paying, high-demand jobs require the kind of education and technical sophistication that developed countries emphasise. These employment opportunities would not exist if industry wasn't standing on the shoulders of public funding and academic performance.
What about healthcare costs saved? For about 15 years, advocates and academicians in the United States have been estimating the cost-savings attributable to medical research. Such savings include money saved from hospitalisations avoided; from productive work gained; or from medical procedures not required as a result of drugs or technologies arising from research. In 1995, Silverstein et al10 examined the annual cost savings that could be attributed to research gains. Their estimate — a cost saving of US$68 billion annually (Box 2) — was felt to be an incomplete summary of the savings. Heading the list of savings were those in the field of psychiatry, where the development of medications for schizophrenia and manic-depressive illness alone saved nearly US$34 billion a year in hospitalisation costs avoided. Next on the list of cost savings were those in the areas of infectious disease, cardiovascular disease and dental health. This 1995 study indicated that for every dollar invested throughout the public and private sectors there was a return of at least 3 to 1 from cost savings alone.
As large as these cost-savings are, they are dwarfed by the return estimated from the value of the lives saved through research. In 1999, the Lasker Foundation, through its Funding First initiative, asked nine academic economists from Columbia, Harvard, Stanford, the University of Chicago and Yale to address new ways to estimate the return on the medical research investment. These investigators chose to focus on the economic value of the increase in life expectancy, and the impressive decline in mortality due to cardiovascular diseases during the past half-century and, more specifically, between 1970 and 1990. Deaths due to cardiovascular disease — the number-one killer of adults in the United States — have fallen by 50% in the past 40 years, and by 30% between 1970 and 1990 (Box 3). Using the number of lives saved in the 1970–1990 interval, multiplied by the monetary value of a life (or a life-year) obtained from standard methodologies for such an estimate, these economists came up with a dollar value for this improved longevity. For cardiovascular diseases this value is attributable in significant part to medical research advances in areas such as thrombosis prevention, blood pressure lowering, control of serum cholesterol, and coronary angioplasty and thrombolysis.
Their work, published first in the report Exceptional returns,4 contains some dramatic findings. First, increases in life expectancy in the United States between 1970 and 1990 were worth roughly US$2.8 trillion dollars a year. This huge sum represents a rate of return on the research investment of greater than a hundred to one! Second, reduced mortality from cardiovascular disease alone was estimated to be worth US$1.5 trillion a year. Third, improvements in life expectancy account for nearly half of the actual gain in US living standards during the past 50 years. Fourth, the likely returns from future medical research are so high that the pay-off for any plausible portfolio of investments will be enormous. For example, research that would lead to reducing cancer deaths by as little as 10% would be worth US$4 trillion.
I was stunned by these results. I knew, of course, that research had given us longer and more productive lives. But I was always taught to consider these outcomes as incalculable. To have an economic value put on our national investment and to find that it was so large was surprising and exhilarating.
Now, let me try to extrapolate some of this information to Australia — a highly developed country like the United States, with similar profiles in life expectancy and major causes of morbidity and mortality. Australia has a number of outstanding universities, medical schools, and research institutes. Your federal government has committed itself to doubling the budget of the National Health and Medical Research Council (NHMRC) in the five-year period between 1999 and 2004.
So much for similarities. There are also major differences. Your current federal government investment in medical research, about A$11 per capita per year, lags well behind that of a number of other developed countries, including Switzerland, Denmark, Japan, Sweden, the United Kingdom and the Netherlands.11 It is less than 10% of the per-capita investment in the United States. Australia's biotechnology and pharmaceutical industries are less robust than those of some of the countries forementioned. The NHMRC infrastructure and the funds that support it appear less than adequate for the task. Finally, Australian medical scientists are generally not willing to speak out to politicians or to the public on behalf of research. Yet scientists know the subject better than anyone else, and politicians want to hear from people who know what they're talking about. I've been told repeatedly by US senators that if we scientists won't come and tell Congress what we want them to do, we have forfeited our right to complain when unfavourable actions are taken.
I address these issues as challenges to be met, not as criticisms. Your research enterprise is young, as is your country. Based on the scientific traditions you've already established and the commitments you've made and are making, I'm confident that these issues will be addressed and will be solved.
Let me close with a few forward-looking comments. Media in my country are filled these days with hyperbolic phrases such as "the days of molecular medicine", "the decade of the human genome project" and "the century of the brain". These words and others like them convey a sense of the excitement surrounding medical science today and in the future. But it may be worth noting that Lewis Thomas — physician, scientist, philosopher and author — wrote 20 years ago: "It is not that there is more to do, there is everything to do. Biological science, with medicine bobbing somewhere in its wake, is under way, but only just under way."12 When we reflect on the major health problems that still confront us, such as congestive heart failure, most cancers, diabetes, asthma and schizophrenia, it's important that we accept humbly the truth of Thomas's message that we are still just barely under way.
As I travel abroad, I am reminded how small today's world is and how important it is that we be part of that world. Not just part of our own institution or our own state or country. Will Durant, the historian, wrote many years ago: "The health of nations is more important than the wealth of nations."13 Those of us who live in countries like the United States and Australia, where we have both health and wealth, must pay far more attention, I believe, to people in less well developed countries than we have to date. First, because the health problems that ravage those countries (malaria, AIDS, malnutrition, parasitic disease) demand humane attention from humane societies. Second, because diseases of the so-called "Third World" are increasingly capable of becoming diseases of the "First World". And, third, because improving the health of people in these countries will increase their wealth, and by so doing permit the governments of these countries to offer better lives to their citizens. After all, it is better, longer, healthier lives that we all want for ourselves, our families and the world's people. And it is better, longer and healthier lives that we, as medical researchers, work towards and are dedicated to.
1: Funding of health research in the United States (1999 financial year), by funding source (in millions)7
2: Annual health costs saved through medical research10*
Category of illness |
Annual savings (US$ billion) |
||||||||||
Psychiatric |
33.9 |
||||||||||
Infectious |
12.5 |
||||||||||
Cardiovascular |
12.0 |
||||||||||
Dental |
3.8 |
||||||||||
Metabolic/endocrine |
2.9 |
||||||||||
Cancer |
1.1 |
||||||||||
Immunological |
1.1 |
||||||||||
Gastrointestinal |
0.9 |
||||||||||
Total |
68.2 |
||||||||||
*Reproduced with permission from Silverstein SC, Garrison HH, Heinig SJ. A few basic economic facts about research in the medical and related life sciences. FASEB J 1995; 9: 833-840. |
|||||||||||
3: Declining mortality in the United States, by cause of death, 1950–19943*
* Reproduced with permission from Cutler DM, Kadiyala S. The economics of better health: the case of cardiovascular disease. Published on the Lasker Foundation website. (From the National Center for Health Statistics, unpublished data.)
Received 7 June 2002, accepted 5 August 2002
- Leon E Rosenberg1
- Department of Molecular Biology, Princeton University, Princeton, New Jersey, USA.
- 1. Perutz M. Nobel Prize laureate for chemistry, 1962. Available at <http://www.medschool.lsumc.edu/bioc/websites/structuralbiochem.htm>. Accessed 26 August 2002, no longer available.
- 2. Roosevelt FD. Quotation from speech at National Cancer Institute, Bethesda; 31 October 1940. Available at: <http://www.nih.gov/about/director/031495.htm>. Accessed 29 August 2002, no longer availabe.
- 3. Exceptional returns: the economic value of America's investment in medical research. Available at: <http://www.laskerfoundation.org/reports/pdf/exceptional.pdf>. Accessed 26 August 2002.
- 4. Strickland SP. Politics, science, and dread disease. Cambridge, MA: Harvard University Press, 1972.
- 5. Investing in health: the unfinished business of medical research. Available at: <http://www.laskerfoundation.org/reports/pdf/invest.pdf>. Accessed 26 August 2002.
- 6. Szent-Györgyi A. Nobel Prize laureate for physiology or medicine, 1937. Available at: <http://www.bartelby.com/63/42/3242.html>. Accessed 30 August 2002.
- 7. Funding of health research in the US. (FY 1999). Available at: <http://www.researchamerica.org>. Accessed 26 August 2002.
- 8. Pharmaceutical Research and Manufacturers of America. PhRMA industry profile 2002. Appendix. Detailed results from the PhRMA annual membership survey. Available at: <http://www.phrma.org/publications/publications/profile02/index.phtml>. Accessed 26 August 2002, no longer available.
- 9. Biotechnology Industry Organization. <http://www.bio.org>.
- 10. Silverstein SC, Garrison HH, Heinig SJ. A few basic economic facts about research in the medical and related life sciences. FASEB J 1995; 9: 833-840.
- 11. Wills PJ (chairman). The virtuous cycle: working together for health and medical research. Health and medical research strategic review (the Wills Report). Canberra: Commonwealth of Australia, 1999.
- 12. Thomas L. Late night thoughts on listening to Mahler's ninth symphony. New York: Viking Press, 1983.
- 13. Durant W. Will Durant quotations. Available at: <http://www.memorablequotations.com/durant.htm>. Accessed 26 August 2002.
Abstract
The United States will invest nearly US$70 billion (US$260 per capita) on medical research this year, more than half of which will be sponsored by the biopharmaceutical industry.
This investment has been shown to provide major gains in basic, disease-oriented and patient-oriented research. It also provides a huge economic return on investment — whether measured in terms of jobs created, health costs saved, or the dollar value of lives saved.
Australia, whose investment in medical research is less than 10% that of the United States, should increase its national commitment.