




The supply of general practitioners is pivotal to the delivery of healthcare to rural and remote communities in Australia. Currently, there continues to be an undersupply of rural doctors, despite implementation at all levels of medical education, training and practice of specific regulatory and incentive-based programs and initiatives to enhance rural medical workforce recruitment and retention.1-3 While most effort to date has focused on recruitment, medical workforce retention has received significantly less attention in Australia, with few detailed empirical studies performed (notable exceptions are those of Kamien4 and Hays et al5). There has also been little attempt to distinguish between the factors influencing rural medical workforce recruitment and those affecting retention.6
The 1998 review of general practice recommended the payment of retention grants based on length of service and rural location as one means of encouraging GPs to remain longer in rural and remote practice than they do now. Funding for these grants was provided in the 1999–2000 Budget.1 However, the formulas for allocating these retention grants proved to be contentious. This was largely because of a lack of empirical evidence identifying (i) the factors most relevant in determining how long a GP would remain in a rural or remote location, (ii) the relative weighting of each retention factor, and (iii) whether the weightings varied in significance in different rural and remote settings.
Consequently, the specific objectives of our study were:
to identify which retention factors are most important in the decision to stay in practice in a rural or remote community;
to develop and test an empirically derived measure (rather than an ordinal ranking) for determining the importance of selected retention factors; and
to determine whether, and if so in what ways, the weightings attributed to each retention factor vary according to the remoteness of the practice and other practitioner characteristics.
The two classifications of rurality and remoteness used in our study are compared in Box 1.
In September 2001, we conducted a national survey of GPs practising in rural and remote communities in April–June 2001. Our survey comprised a stratified sample of 1400 GPs obtained from the Health Insurance Commission after approval from the Statistical Clearing House.10 To ensure a representative spread across the diversity of rural and remote communities, the sample was stratified according to the Rural, Remote and Metropolitan Areas (RRMA) classification categories 3–7 (Box 1).8
An extensive search of the current Australian and international literature was conducted to identify the factors influencing rural medical workforce retention.6 In general, factors affecting retention and turnover fall into three broad categories: professional issues, social factors relating to personal characteristics and the family, and external factors relating to the community and its geographical location.
GPs were asked to consider the importance of six professional, social or community workforce retention factors:
The variety of rural practice, including procedural activity;
The availability of professional support from local, well qualified colleagues and specialists, and from professional organisations through continuing medical education (CME);
Good on-call arrangements, including time off for holidays;
Local availability of services, including education for children and opportunities for spouse employment;
Proximity to a city or large regional centre; and
Local geographic attractions, such as proximity to the coast or national parks, or opportunities for a rural lifestyle.
The Bradley–Terry model of paired comparisons was used to elicit the importance of workforce retention factors. The model is a logit form of a log-linear model for quasi-symmetry.11 The model parameters represent the relative probability of selection for each retention factor compared with a reference choice.
The paired-comparisons technique requires respondents to evaluate all possible pairs of (in our study) retention factors, and, in each case, to choose one over the other. Each factor is paired with every other factor in all possible combinations, with no equal choices allowed. To reduce bias, pairs of alternative retention factors are arranged so that each appears equally on the right and left side of the questionnaire page, alternates from right to left, and does not appear consecutively, but rather is spaced as far apart as possible.12
Given a set of n alternatives, n(n–1)/2 comparisons must be made by each respondent. To avoid the effect of respondent fatigue, only a relatively small number of factors can be included.
The result was a preference scale of alternatives as rated by the participants. Importantly, both the rank order of importance of retention factors and an estimate of the interval separating the factors were obtained. Because the values for each factor reflect the characteristics of the data, the origin of the scale is arbitrary. To facilitate comparison, the scaling is transformed to a base of zero by ranking the least important factor as zero.
A total of 677 usable questionnaires was returned from the 1344 eligible practising rural and remote GPs, representing a 50% response rate (Box 2).
The results of the paired-comparison analyses (Figures A–D) are shown in Box 3. The vertical axes represent an open-ended index of the perceived importance of each factor relative to the reference factor "proximity to city or large regional centre", which is set at zero. Positive values of the index indicate greater perceived importance. In interpreting our findings, priority was given to the rank order of factors and the magnitude of the differences in the parameter estimates.
Some indication of whether the differences in importance could be due to chance was obtained from 95% CIs, but to preserve clarity these are not shown in Box 3. Statistical significance was of secondary importance to order and magnitude of the difference in values. (Detailed tabular versions of the Figures in Box 3, including CIs, are available from us on request.)
Until the recent introduction of retention payments, relatively little had been done to encourage rural doctors to stay in rural practice. Although there is undoubtedly some overlap between the factors influencing recruitment and retention, important differences exist that warrant consideration.6,13 Ours is the first comprehensive Australian study identifying the importance of factors influencing how long rural GPs are likely to stay in their communities. Our results support the assertion that, while "the decision to locate in a rural practice setting occurs largely from outside that setting . . . the decision to remain takes place from within the practice setting and arises from the stream of experience there".14
The overwhelming importance of professional factors as determinants of length of practice in rural areas is confirmed. The key workforce problem for rural doctors is inability to get time away for recreational leave and family considerations, and for emergency relief and relief to complete CME programs. The difficulties providing an after-hours service and ensuring reasonable on-call arrangements relate to the size and location of the community. Currently, the problem is most acute in the smaller rural and remote communities. In the absence of good on-call arrangements and professional support, the unrelenting nature of after-hours care imposes an excessive workload, with negative effects both on GPs' (and their families') health and well-being, and on their opportunities to enjoy their rural location.
Currently, rural retention grants provide some reward for duration of stay in a practice. The results of our study provide a sound empirical basis for weighting the retention-grant allocation formulas to ensure that these grants reflect the varying importance of factors determining length of stay.
Additionally, however, a strategic, long-term solution is required to ensure acceptable on-call and after-hours arrangements and to provide appropriate professional support, thereby minimising the onset of triggers that may lead to doctors leaving a rural practice prematurely. Interventions not affecting on-call and related professional issues will not solve the key problem. A broad strategic solution incorporating several measures is required, including:
Recruiting more rural doctors to help provide a reasonable on-call ratio and ensure comprehensive after-hours care. History shows, however, that the recruitment of rural doctors is no easy task. Recruiting female doctors (who now comprise over half of the medical school intake and have a different set of expectations in terms of practice activities) will be particularly challenging.
An appropriate locum strategy guaranteeing the provision of locums at an affordable price. To date, governments, through Rural Workforce Agencies and Divisions of General Practice, have focused on providing locums as the mechanism for providing leave. However, a locum-based strategy alone is not a sustainable long-term solution, particularly given the large number of locums required to provide adequate relief for all doctors working in rural and remote Australia. Moreover, use of locums raises issues about suitability of their training for rural and remote practice, continuity and standards of patient care, practice maintenance and the inevitable requirement to source the bulk of these locums from overseas.
The development of regional medical practice models in appropriate rural settings. This may facilitate a reduction in on-call ratios and enhance opportunities for professional support. In this way, communities currently supporting a solo practice can support another doctor, two-GP towns can become three-GP towns, and so on, so that the facility to cover after-hours and relieve pressure is built into the local practice staffing and organisation arrangements.15
The importance attributed to variety of rural practice as a factor influencing the length of time in rural practice should not be overlooked. Many doctors move to rural areas because of the opportunity to practise procedural and comprehensive care. The factors that determine opportunities to engage in a variety of rural medical practices are complex, including other support staff, availability of facilities, changing technologies, improving transportation and changed community expectations. Nonetheless, it should be recognised that health policies (driven largely by economic imperatives) resulting in reductions in procedural and hospital activity not only affect the length of time that GPs will remain in practice, but also the ability to recruit doctors to rural and remote practice. Similarly, the disincentive of increasing medical indemnity payments for rural medical proceduralists is now widely recognised.
Measures to improve rural medical workforce retention must not be introduced at the expense of a viable and attractive practice income for existing local doctors. Hence, any move to relieve onerous on-call commitments by bringing another doctor into a small town, normally serviced adequately by one GP, must take into account the effect on (or threat to) the economic sustainability of the practice.
The challenge is to develop an integrated rural medical workforce retention strategy which
takes account of the nature, complexity, and context of rural and remote general practice;
provides professional support and remuneration appropriate to skills and responsibilities; and
enables the doctor to spend a reasonable amount of time away from the practice.
Such a strategy will not only meet the needs of existing rural practitioners, but also serve to enhance the attractiveness of rural practice to prospective rural practitioners.
1: Comparison of the categories for rural and remote of the Rural, Remote and Metropolitan Areas (RRMA) classification and the Accessibility/Remoteness Index of Australia (ARIA)7-9
RRMA classification |
ARIA categories |
||||||||||
Rural zone |
|||||||||||
RRMA 3 – Large rural centre (population, 25 000–99 000) |
Highly accessible (ARIA score, 0–1.84) — relatively unrestricted accessibility to a wide range of goods and services and opportunities for social interaction |
||||||||||
RRMA 4 – Small rural centre (population, 10 000–24 999) |
Accessible (ARIA score, > 1.84–3.51) — some restrictions to accessibility of some goods, services and opportunities for social interaction |
||||||||||
RRMA 5 – Other rural area (population, < 10 000) |
Moderately accessible (ARIA score, > 3.51–5.80) — significantly restricted accessibility to goods, services and opportunities for social interaction |
||||||||||
Remote zone |
|||||||||||
RRMA 6 – Remote centre (population, 5000 or more) |
Remote (ARIA score, > 5.80–9.08) — very restricted accessibility of goods, services and opportunities for social interaction |
||||||||||
RRMA 7 – Other remote area (population, < 5000) |
Very remote (ARIA score, > 9.08–12) — very little accessibility of goods, services and opportunities for social interaction |
||||||||||
2: General practitioner sample and number (%) of valid responses by Rural, Remote and Metropolitan Areas (RRMA) classification
RRMA category |
Eligible GPs* |
Responses† |
|||||||||
3 |
386 |
168 (43.5%) |
|||||||||
4 |
388 |
189 (48.7%) |
|||||||||
5 |
387 |
227 (58.7%) |
|||||||||
6 |
86 |
41 (47.7%) |
|||||||||
7 |
97 |
52 (53.6%) |
|||||||||
Total |
1344 |
677 (50.4%) |
|||||||||
* Reasons such as "return to sender", "moved from place of residence" reduced the sample from 1400 to 1344 GPs. † Usable returned questionnaires. |
|||||||||||
3: Relative importance of each of six factors in GPs' decisions to remain in rural practice
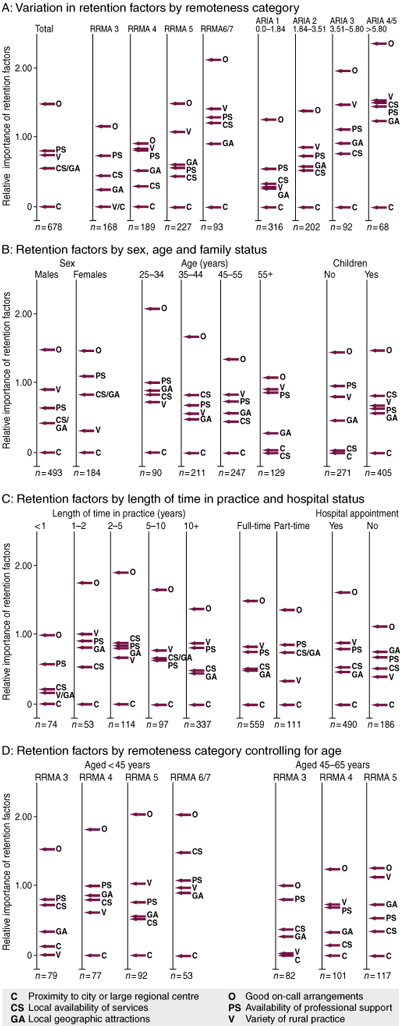 A: Importance of retention factors by rurality or remoteness. Both RRMA categories and the Accessibility/Remoteness Index of Australia (ARIA) were used.8,9 Some categories (invariably RRMA 6 and 7, and ARIA 4 and 5) were combined if there were too few responses for statistical reliability. Although the RRMA and ARIA categories are not strictly comparable (Box 1), the results display significant consistency for both measures of remoteness.
B, C: Retention factors by demographic and practice characteristics. These identified a somewhat different order of priorities — most notably for younger, female GPs, with children or part-time.
D: Retention factors by age and rurality or remoteness. Because of small numbers, only two age groups were used.
|
- John S Humphreys1
- Judith A Jones2
- Michael P Jones3
- Paul R Mara4
- 1 Monash University School of Rural Health, North Bendigo, VIC.
- 2 Jones & Just, Mt Kuringai, NSW.
- 3 Health Connections, Gundagai, NSW.
This research was funded through the Commonwealth Department of Health and Ageing General Practice Branch. Particular thanks go to Gordon Calcino, Naarilla Hirsch and Angela Mikalauskas for their assistance in expediting access to Health Insurance Commission data.
None declared.
- 1. Commonwealth Department of Health and Family Services. Changing the future through partnerships. The Report of the General Practice Strategy Review. Canberra: Department of Health and Family Services, 1998.
- 2. Department of Health and Aged Care. General Practice in Australia 2000. Canberra: Department of Health and Aged Care, 2000.
- 3. Department of Health and Aged Care. The Australian Medical Workforce. Occasional Papers: New series No.12. Canberra: Department of Health and Aged Care, 2001.
- 4. Kamien M. Staying in or leaving rural practice: 1996 outcomes of rural doctors' 1986 intentions. Med J Aust 1998; 169: 318-321.
- 5. Hays R, Veitch C, Cheers B, Crossland L. Why doctors leave rural practice. Aust J Rural Health 1995; 5: 198-203.
- 6. Humphreys J, Jones J, Jones M, et al. A critical review of rural medical workforce retention in Australia. Aust Health Rev 2001; 24: 91-102.
- 7. Department of Primary Industries and Department of Human Services and Health. Rural, Remote and Metropolitan Areas Classification. Canberra: AGPS, 1994.
- 8. Australian Bureau of Statistics. Outcomes of ABS Views on Remoteness Consultation, Australia. Information Paper. Canberra: ABS, 2001. (Catalogue No. 1244.0.00.001.)
- 9. Department of Health and Aged Care. Measuring remoteness: Accessibility/Remoteness Index of Australia (ARIA). Occasional Papers: New series No.14. Canberra: Department of Health and Aged Care, 2001.
- 10. Colledge M, Starick R. Australian Commonwealth Government Statistical Clearing House: vehicle for reducing response load and improving survey quality. Int Stat Rev 2000; 48: 221-231.
- 11. Agresti A. Categorical data analysis. New York: John Wiley & Sons, 1991.
- 12. Wells AJ. Optimal presentation orders for the method of paired comparisons. Br J Math Stat Psychol 1991; 44: 181-193.
- 13. National Rural Health Association, 1998. Physician recruitment and retention, Issue Paper, November 1998 Available at: http://www.nrharural.org/dc/issuepapers/ipaper13.html (accessed March 2002).
- 14. Cutchin M. Community and self: concepts for rural physician integration and retention. Soc Sci Med 1997; 44: 1661-1674.
- 15. Down G, Jefferies F, Seward M. Towards Northern Wheatbelt GP sustainability: a study by WACRRM for Northern Wheatbelt communities. Perth: University of Western Australia; 2000.
Abstract
Objectives: To ascertain which factors are most significant in a general practitioner's decision to stay in rural practice and whether these retention factors vary in importance according to the geographical location of the practice and GP characteristics.
Design: National questionnaire survey. The method of paired comparisons was used to describe the relative importance of the retention items.
Setting: Non-metropolitan Australia, September 2001.
Participants: A stratified sample of all rural GPs practising during April–June 2001.
Main outcome measures: A rank ordering of factors influencing how long GPs stay in rural practice, and an index of their relative perceived importance.
Results: Professional considerations — overwhelmingly, on-call arrangements — are the most important factors determining GP retention in rural and remote areas. Rural doctors consistently ranked on-call arrangements, professional support and variety of rural practice as the top three issues, followed by local availability of services and geographical attractiveness. Proximity to a city or large regional centre was the least important factor. Retention factors varied according to geographical location and GPs' age, sex, family status, length of time in the practice, and hospital duties.
Conclusions: A broad, integrated rural retention strategy is required to address on-call arrangements, provide professional support and ensure adequate time off for continuing medical education and recreation.