




The known: Residential wood heating is a major source of hazardous air pollution in many Australian cities and towns.
The new: In Armidale, a regional NSW city of 24 504 people, 14 premature deaths per year are attributable to air pollution from wood heaters. This corresponds to 210 lost years of life, at an estimated cost of $10 930 per heater per year.
The implications: Effective measures to reduce wood heater pollution are needed, including public education about the damage to health caused by wood smoke, providing incentives to switch to less polluting heating, and regulations that limit the use of wood heaters.
Domestic wood heating is a major source of air pollution in Australia, including fine particulate matter (particles less than 2.5 μm aerodynamic diameter, PM2.5), generally regarded as the most hazardous air pollutant1,2,3 (Supporting Information, part 1). For the 5.6 million residents of the Sydney–Newcastle–Wollongong region and surrounding areas, 420 premature deaths per year are attributed to PM2.5 pollution;4 in this Greater Sydney Metropolitan Region, wood heaters contribute 24–42% of anthropogenic PM2.5, compared with 7–17% for power stations and 17–19% for road vehicles.4,5,6 In Tasmania, 65 premature deaths per year were attributed to wood heater pollution during 2010‒2019, compared with four deaths per year ascribed to landscape fire smoke.7 However, wood smoke pollution from the extraordinary bushfires in eastern Australia was responsible for an estimated 417 excess deaths during 1 October 2019 ‒ 10 February 2020.8
Larger proportions of households in regional Australia use wood heating than in metropolitan areas. Air pollution monitoring in regional towns is generally limited, leading to misperception of the magnitude of wood heater pollution and the associated health burden. In 2018, an NSW government air pollution monitoring station was installed in Armidale (Northern Tablelands; population, 24 504), complemented by a network of eleven calibrated low cost monitors,9 enabling detailed characterisation of population PM2.5 exposure by season. In winter, cold, frosty nights are typical for Armidale, and about 40% of households use wood heating, the main source of air pollution in the city.9 Air pollution in Armidale exceeded the national daily PM2.5 standard (25 µg/m3) on 32 days in 2018; all exceedances were attributable to winter wood heater pollution10 (Supporting Information, part 2).
The aim of our study was to estimate the numbers of premature deaths, and the years of life lost and their associated health costs, attributable to wood heater pollution in Armidale, based on PM2.5 levels measured during 1 May 2018 – 30 April 2019.
Methods
We used autovariogram kriging to interpolate daily mean PM2.5 measurements based on data from the Armidale monitoring network, comprising the NSW government air pollution monitoring station equipped with a TEOM 1405 with filter dynamics measurement system (ThermoFisher)11 and ten of eleven calibrated low cost monitors (PurpleAir); we excluded data from one monitor that appeared to be faulty.9 The interpolated measurements were aggregated to estimate daily population‐weighted PM2.5 exposure (DPWP25) for the Armidale Statistical Area 2 during 1 May 2018 – 30 April 2019, according to the 2016 usual resident population. We then defined two periods by examining the data: the wood heater pollution period and a background period not usually affected by wood smoke. For the wood heater pollution period, population‐weighted wood smoke PM2.5 exposure was defined as daily exposure exceeding the background period mean (further details: Supporting Information, part 3).
We estimated the number of premature deaths attributable to wood heater emissions using methods similar to those of a recent analysis of the health impacts of ambient smoke in Tasmania7 (Supporting Information, sections 3‒6). We converted mean daily population‐weighted wood smoke PM2.5 exposure during the wood heater pollution period to mean annual wood heater PM2.5 population exposure (AWPE), and then used the Global Exposure Mortality Model (GEMM)12 to estimate the increase in number of premature deaths by sex and 5‐year age group and calculate years of life lost (YLL) and reductions in life expectancy (Supporting Information, part 5). We also estimated the mortality parameters using an alternative risk function, the Health Risks of Air Pollution in Europe (HRAPIE) model, in which the risk is defined as 1 for people under 30 years of age and 1.062AWPE/10 for people over 30.13
The financial cost associated with the impact on mortality was estimated using a value of statistical life year of $213 000 for the first year of life lost, and discounted 3% per year for subsequent years lost, as recommended by the Office of Best Practice Regulation.14
All analyses were undertaken in R 4.0.2 (R Project for Statistical Computing).
Ethics approval
Our analysis of publicly available data did not require formal ethics approval.
Results
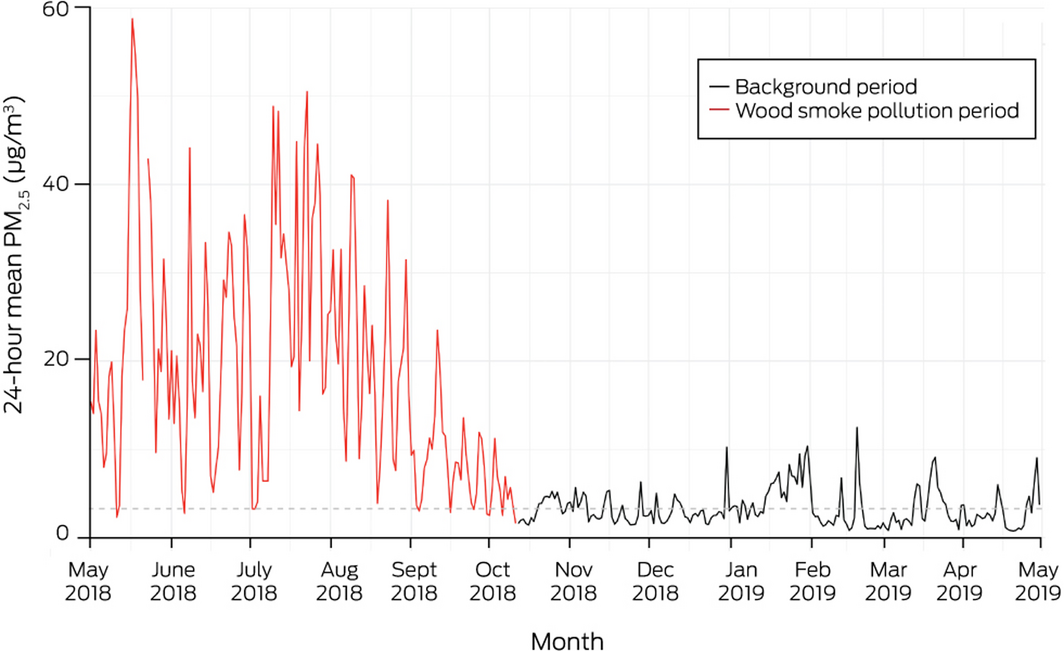
The population‐weighted PM2.5 time series for Armidale, 1 May 2018 – 30 April 2019, is shown in Box 1. The two time periods defined were the wood heater pollution period (164 days: 1 May – 11 October 2018) and the background period (12 October 2018 – 30 April 2019). Mean DPWP25 was 3.1 µg/m3 during the background period and 18.8 µg/m3 during the wood heater pollution period; the mean daily population‐weighted wood smoke PM2.5 exposure for the wood heater pollution period was 15.6 µg/m3 (AWPE, 7.0 µg/m3) (Supporting Information, section 7).
Using the GEMM, we estimated that 14 premature deaths (95% confidence interval [CI], 11.7–16.6 deaths) per year were attributable to wood heater‐related PM2.5 exposure, corresponding to 210 (95% CI, 172–249) YLL per year and, longer term, to the loss of 364 (95%, 297–432) days of life expectancy at birth. The estimated cost of the YLL was $32.8 million (95% CI, $27.0‒38.5 million), or $10 930 (95% CI, $9004–12 822) per wood heater per year. Applying the HRAPIE model, we estimated an annual cost of $4928 per wood heater (Box 2; Supporting Information, section 7).
Discussion
The estimated numbers of premature deaths and YLL attributable to wood heater PM2.5, and the associated cost, indicate that wood heater pollution should be reduced in Armidale and other locations where wood heating is a major source of air pollution.
A decade ago, research commissioned by the NSW government found that wood heater pollution in NSW caused $8 billion in health costs over 20 years, and that this could be reduced by 75% by requiring that wood heaters be removed when houses are sold and not permitting the installation of new units.15 For 35 heaters in New Zealand satisfying requirements stricter than the current AS/NZS 4013 standard, mean real life emissions were 6.5 g particulate matter per kg dry wood, eight times as high as the mean of 0.85 g/kg during AS/NZS testing.16,17 This illustrates that newer wood heaters are little better than those tested in Tasmania in 2006 and 2007 (mean real life emissions, 9.4 g/kg).18
Limited awareness of the health costs of wood heater pollution (and the magnitude of the emissions) has hindered the development of effective policy. Governments and the public need accurate information to make informed decisions. The vice‐president of the Rural Doctors Association of Victoria, Rob Phair, wrote in September 2020:
Doctors can make a big contribution in discussions about air pollution with our patients, local communities and government. The discussion about wood heaters should resemble the discussion about tobacco smoking… Smoking in public places is recognised as harmful to public health. The same recognition should be extended to domestic wood heaters.19
In 2020, the Australian Medical Association Victoria supported calls for a buyback scheme to remove wood heaters from homes20 because they were estimated to cause $8 billion in health costs over ten years in Victoria.21 In 2019, the authors of an overview of air quality research funded by the National Environmental Science Program on behalf of the Australian Department of the Environment and Energy proposed a Clean Air Plan for Sydney; one priority was legislation that “works towards eliminating the use of wood‐heaters in urban areas”.22 This would entail requiring wood heaters to be removed when homes are sold, not permitting the installation of new heaters, education programs, assistance for residents affected by other people’s wood smoke, and subsidies to encourage switching to efficient heating with lower emissions. A national survey by Asthma Australia of 25 000 people in November 2020 found that most people, particularly those with asthma, support phasing out wood heaters and using better, healthier alternatives.23
The Wood Heater Replacement Program in Launceston (2001‒2004) was part of a package that reduced winter PM10 pollution by an estimated 16.6 µg/m3 and was associated with substantial health benefits, reducing the numbers of wintertime respiratory (by 28%) and cardiovascular disease deaths (by 20%), and annual all‐cause mortality in males (by 11.4%). The program cost about $29 per resident.24 However, progress stalled once subsidies ceased and residents installed new wood heaters (Supporting Information, section 8).
Our analysis of the health effects of wood heaters was restricted to the risk of premature death. Other adverse health outcomes of air pollution include premature birth, lower birthweight, stroke, neurodegenerative disease, diabetes, deep venous thrombosis, and cardiovascular and lung disease25 (Supporting Information, section 9). A recent review found that both short and long term exposure to air pollution may be important aggravating factors for coronavirus disease 19 (COVID‐19) transmission, severity, and lethality.26 Support for reducing wood heater pollution could be provided as part of a COVID‐19 economic recovery package, similar to grants that were available for building new homes or undertaking renovations costing more than $150 000.27 Subsidies for replacing wood heaters with cleaner options (in conjunction with upgraded insulation, when necessary) would provide additional employment, improve health, reduce heating costs for households that buy firewood, and help slow global warming (further discussion of policy implications: Supporting Information, section 10).
Limitations
Estimates of the impact of air pollution are highly sensitive to the choice of exposure risk function. The 2013 HRAPIE meta‐analysis was based on eleven studies of PM2.5 and mortality,13 whereas the 2018 GEMM included 41 cohorts from 16 countries;12 its estimates may therefore be more robust (Supporting Information, section 11).
Conclusion
Effective policies are needed to reduce wood heater pollution, including public education supported by health professionals about the effects on health of wood smoke, subsidies that encourage residents to switch to efficient, less polluting home heating (perhaps as part of an economic recovery package), and regulatory changes.
Box 2 – Estimated number of premature deaths, years of life lost, financial cost, and loss of life expectancy attributable to domestic wood heater pollution in Armidale, 1 May 2018 – 30 April 2019*
|
Risk model |
Premature deaths |
Years of life lost (YLL) |
Financial cost of YLL |
Lost life expectancy |
|||||||||||
|
|
|||||||||||||||
|
GEMM |
14.2 (11.7–16.6) |
210.3 (171.7–248.9) |
32.8 (27.0–38.5) |
364 (297–432) |
|||||||||||
|
HRAPIE |
6.7 (4.4–8.9) |
90.4 (58.9–120.1) |
14.8 (9.7–19.5) |
162 (105–216) |
|||||||||||
|
|
|||||||||||||||
|
GEMM = Global Exposure Mortality Model;12 HRAPIE = Health Risks of Air Pollution in Europe.13 * Estimates by sex are included in the online Supporting Information, part 8. |
|||||||||||||||
Received 18 November 2020, accepted 18 June 2021
- Dorothy L Robinson1
- Joshua A Horsley2
- Fay H. Johnston3
- Geoffrey G Morgan4
- 1 University of New England, Armidale, NSW
- 2 Sydney Medical School, University of Sydney, Sydney, NSW
- 3 Menzies Institute for Medical Research, University of Tasmania, Hobart, TAS
- 4 University Centre for Rural Health, Lismore, NSW
We thank the NSW Office of Environment and Heritage for installing an air pollution monitoring station in Armidale and assisting with the installation of PurpleAir units (for checking and calibration) on the roof of the monitoring station, and the Armidale Regional Council for purchasing and installing further PurpleAir units.
No relevant disclosures.
- 1. European Environment Agency. Air quality in Europe: 2020 report (EEA report no. 09/2020). Luxembourg: Publications Office of the European Union, 2020. https://www.eea.europa.eu/publications/air‐quality‐in‐europe‐2020‐report (viewed Apr 2021).
- 2. The Lancet. Ambient particulate matter pollution: Level 4 risk. In: Global Burden of Disease (GBD) cause and risk summaries (2019 data). Lancet 2020; 396: S228–S230. https://www.thelancet.com/pb‐assets/Lancet/gbd/summaries/risks/ambient‐particulate‐matter‐pollution.pdf (viewed Apr 2021)
- 3. The Lancet. Ambient ozone pollution: Level 3 risk. In: Global Burden of Disease (GBD) cause and risk summaries (2019 data). Lancet 2020; 396: S232–S233. https://www.thelancet.com/pb‐assets/Lancet/gbd/summaries/risks/ambient‐ozone‐pollution.pdf (viewed Apr 2021).
- 4. Broome RA, Powell J, Cope ME, Morgan GG. The mortality effect of PM2.5 sources in the Greater Metropolitan Region of Sydney, Australia. Environ Int 2020; 137: 105429.
- 5. Chang LTC, Scorgie Y, Duc HN, et al. Major source contributions to ambient PM2.5 and exposures within the New South Wales Greater Metropolitan Region. Atmosphere 2019; 10: 138.
- 6. Department of Planning, NSW Clean Air Strategy 2021–30. Draft for consultation. Mar 2021. https://www.environment.nsw.gov.au/topics/air/clean‐air‐strategy/draft‐nsw‐clean‐air‐strategy‐public‐consultation (viewed Apr 2021).
- 7. Borchers‐Arriagada N, Palmer AJ, Bowman DMJS, et al. Health impacts of ambient biomass smoke in Tasmania, Australia. Int J Environ Res Public Health 2020; 17: 3264.
- 8. Borchers Arriagada N, Palmer AJ, Bowman DMJS, et al. Unprecedented smoke‐related health burden associated with the 2019–20 bushfires in eastern Australia. Med J Aust 2020; 213: 282–283. https://www.mja.com.au/journal/2020/213/6/unprecedented‐smoke‐related‐health‐burden‐associated‐2019‐20‐bushfires‐eastern
- 9. Robinson DL. Accurate, low cost PM2.5 measurements demonstrate the large spatial variation in wood smoke pollution in regional Australia and improve modeling and estimates of health costs. Atmosphere 2020; 11: 856.
- 10. Office of Environment and Heritage (NSW). NSW annual air quality statement 2018. June 2019. https://www.environment.nsw.gov.au/research‐and‐publications/publications‐search/nsw‐annual‐air‐quality‐statement‐2018 (viewed Apr 2021).
- 11. Riley ML, Kirkwood J, Jiang N, et al. Air quality monitoring in NSW: from long term trend monitoring to integrated urban services. Air Quality and Climate Change 2020; 54: 44–51.
- 12. Burnett R, Chen H, Szyszkowicz M, et al. Global estimates of mortality associated with long‐term exposure to outdoor fine particulate matter. Proc Natl Acad Sci U S A 2018; 115: 9592–9597.
- 13. World Health Organization (Regional Office for Europe). Health risks of air pollution in Europe: HRAPIE project. Recommendations for concentration–response functions for cost–benefit analysis of particulate matter, ozone and nitrogen dioxide. Copenhagen: WHO, 2013. https://www.euro.who.int/__data/assets/pdf_file/0006/238956/Health_risks_air_pollution_HRAPIE_project.pdf (viewed Apr 2021).
- 14. Office of Best Practice Regulation (Australia). Best practice regulation guidance note. Value of statistical life. Aug 2019. https://www.pmc.gov.au/sites/default/files/publications/value‐of‐statistical‐life‐guidance‐note_0_0.pdf (viewed Apr 2021).
- 15. AECOM Australia. Economic appraisal of wood smoke control measures. Final report. Prepared for the Office of Environment and Heritage. June 2011. https://www.epa.nsw.gov.au/resources/air/WoodsmokeControlReport.pdf (viewed Apr 2021).
- 16. Wilton E. Review: particulate emissions from wood burners in New Zealand. Prepared for the National Institute of Water and Atmospheric Research. Dec 2012. https://niwa.co.nz/sites/niwa.co.nz/files/WoodburnerReportFinal.pdf (viewed Apr 2021).
- 17. Australian Air Quality Group – Woodsmoke. Comparison of real‐life and AS/NZS 4013 lab test results of 35 wood heaters in NZ. July 2021. http://woodsmoke.3sc.net/files/AS-NZS_4013_vs_real_life_in_NZ.pdf (viewed July 2021).
- 18. Meyer CP, Luhar A, Gillett R, Keywood M. Measurement of real‐world PM10 emission factors and emission profiles from woodheaters by in situ source monitoring and atmospheric verification methods. Final Report of Clean Air Research Project 16 for Australian Commonwealth Department of the Environment Water Heritage and the Arts. May 2008. Archived: https://web.archive.org/web/20130430161853/http://environment.gov.au/atmosphere/airquality/publications/pubs/emission‐factor.pdf (viewed Apr 2021).
- 19. Phair R. Wood heaters: the cosy killers. VicDoc (AMA Victoria) [online], Sept 2020. https://vicdoc.partica.online/vicdoc/vicdoc‐september‐2020/features/wood‐heaters‐the‐cosy‐killers (viewed Apr 2021).
- 20. Hope Z. AMA fires up over wood heater buy‐back scheme. The Age (Melbourne), 13 June 2020. https://www.theage.com.au/national/victoria/ama‐fires‐up‐over‐wood‐heater‐buy‐back‐scheme‐20200611‐p5528k.html (viewed Apr 2021).
- 21. Regulatory Impact Solutions. Variation to the waste management policy (solid fuel heating). Policy impact assessment. Prepared for the Environment Protection Authority, Victoria. Nov 2017. https://www.epa.vic.gov.au/‐/media/epa/files/about-epa/what-we-do/piawastemanagementpolicysolidfuelheating.pdf (viewed Apr 2021).
- 22. Paton‐Walsh C, Rayner P, Simmons J, et al. A clean air plan for Sydney: an overview of the special issue on air quality in New South Wales. Atmosphere 2019; 10: 774.
- 23. Asthma Australia. Public would support a “phase‐out” of woodfire heaters [media release]. 18 Mar 2021. https://asthma.org.au/about‐us/media/public‐would‐support‐a‐phase‐out‐of‐woodfire‐heaters (viewed Apr 2021).
- 24. Johnston FH, Hanigan IC, Henderson SB, Morgan GG. Evaluation of interventions to reduce air pollution from biomass smoke on mortality in Launceston, Australia: retrospective analysis of daily mortality, 1994–2007. Br Med J 2013; 346: e8446.
- 25. Thurston GD, Kipen H, Annesi‐Maesano I, et al. A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. Eur Respir J 2017; 49: 1600419.
- 26. Bourdrel T, Annesi‐Maesano I, Alahmad B, et al. The impact of outdoor air pollution on COVID‐19: a review of evidence from in vitro, animal, and human studies. Eur Resp Rev 2021; 30: 200242.
- 27. Australian Government. Economic response to the coronavirus: Home Builder. https://treasury.gov.au/sites/default/files/2021‐04/homebuilderfactsheet2704.pdf (viewed Apr 2021).
Abstract
Objectives: To estimate the annual burden of mortality and the associated health costs attributable to air pollution from wood heaters in Armidale.
Design: Health impact assessment (excess annual mortality and financial costs) based upon atmospheric PM2.5 measurements.
Setting: Armidale, a regional Australian city (population, 24 504) with high levels of air pollution in winter caused by domestic wood heaters, 1 May 2018 – 30 April 2019.
Main outcome measures: Estimated population exposure to PM2.5 from wood heaters; estimated numbers of premature deaths and years of life lost.
Results: Fourteen premature deaths (95% CI, 12–17 deaths) per year, corresponding to 210 (95% CI, 172–249) years of life lost, are attributable to long term exposure to wood heater PM2.5 pollution in Armidale. The estimated financial cost is $32.8 million (95% CI, $27.0–38.5 million), or $10 930 (95% CI, $9004–12 822) per wood heater per year.
Conclusions: The substantial mortality and financial cost attributable to wood heating in Armidale indicates that effective policies are needed to reduce wood heater pollution, including public education about the effects of wood smoke on health, subsidies that encourage residents to switch to less polluting home heating (perhaps as part of an economic recovery package), assistance for those affected by wood smoke from other people, and regulations that reduce wood heater use (eg, by not permitting new wood heaters and requiring existing units to be removed when houses are sold).