




Time to commit to working in respectful partnerships with Indigenous people
During 2006 and 2007, there was much discussion in the media about child sexual assault in Northern Territory Aboriginal communities. In April 2007, the report of the NT Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse, entitled Ampe akelyernemane meke mekarle “Little children are sacred”, was presented to the Chief Minister of the NT Government; it was released to the public in June 2007. The report addressed concerns about child sexual abuse and made recommendations that child abuse and child sexual abuse be designated as issues of urgent national significance by both the Australian and NT governments.1
On 21 June 2007, the then Minister for Families, Community Services and Indigenous Affairs, Mal Brough MP, announced, on behalf of the Australian Government, the Northern Territory Emergency Response (NTER) to protect Aboriginal children in the NT.2 The announcement included, among other measures, alcohol restrictions, welfare reform, compulsory income management, compulsory health checks, banning of pornography, scrapping of the permit system for common areas, and improving housing and community living arrangements. Significantly, legislation was passed by the Australian Parliament suspending Part II of the Racial Discrimination Act 1975 (Cwlth), so that the government’s measures could be imposed in prescribed Aboriginal communities in the NT.3 Part II of the Act prohibits racial discrimination in rights to equality before the law; access to places and facilities, land, housing and other accommodation; and provision of goods and services.
The health impact assessment uses methods endorsed by the World Health Organization.4 It is a predictive tool to assess the potential health impacts of a proposed policy, program or project on the health of a population, and it makes practical recommendations to improve the proposal. It is not an evaluation; rather, by seeking to predict the impacts on the health of affected populations, it has the potential to inform decision making before a proposal is implemented and before negative effects occur. Qualitative and quantitative methods are used to predict the health impact of a given policy on selected health parameters.
The health impact assessment of the NTER is underpinned by the Aboriginal understanding of health and wellbeing. It refers to The dance of life model developed by Professor Helen Milroy, Director of the Centre for Aboriginal Medical and Dental Health at the University of Western Australia.5 This model represents an Aboriginal interpretation of health and illustrates health in its five dimensions — cultural, spiritual, social, emotional and physical — within which are a number of layers reflecting historical, traditional and contemporary influences on health. These five dimensions were examined within the health impact assessment framework.5
In preparing our report, we spoke to more than 250 people affected by the intervention measures. Grandmothers spoke about the humiliation of going “back to the old days” when all decisions were made for them. Mothers spoke about the added burden of trying to buy family groceries using the BasicsCard,6 which can only be used in specified locations. Communities spoke about their hurt when their successful local programs were disregarded by the government. And men everywhere spoke about their despair at being labelled as paedophiles.
The main findings of the report are that:
the intervention could potentially lead to profound long-term damage, with any possible benefits to physical health largely outweighed by negative impacts on psychological health, social health and wellbeing, and cultural integrity;
the increasing levels of mistrust caused by the Howard Government’s ill conceived and rushed implementation of the intervention will continue to compromise the Rudd Government’s ability to work in partnership with Aboriginal communities to achieve shared objectives; and
the potential negative impacts of the intervention may be minimised, but only if governments commit to working in respectful partnerships with Indigenous people.
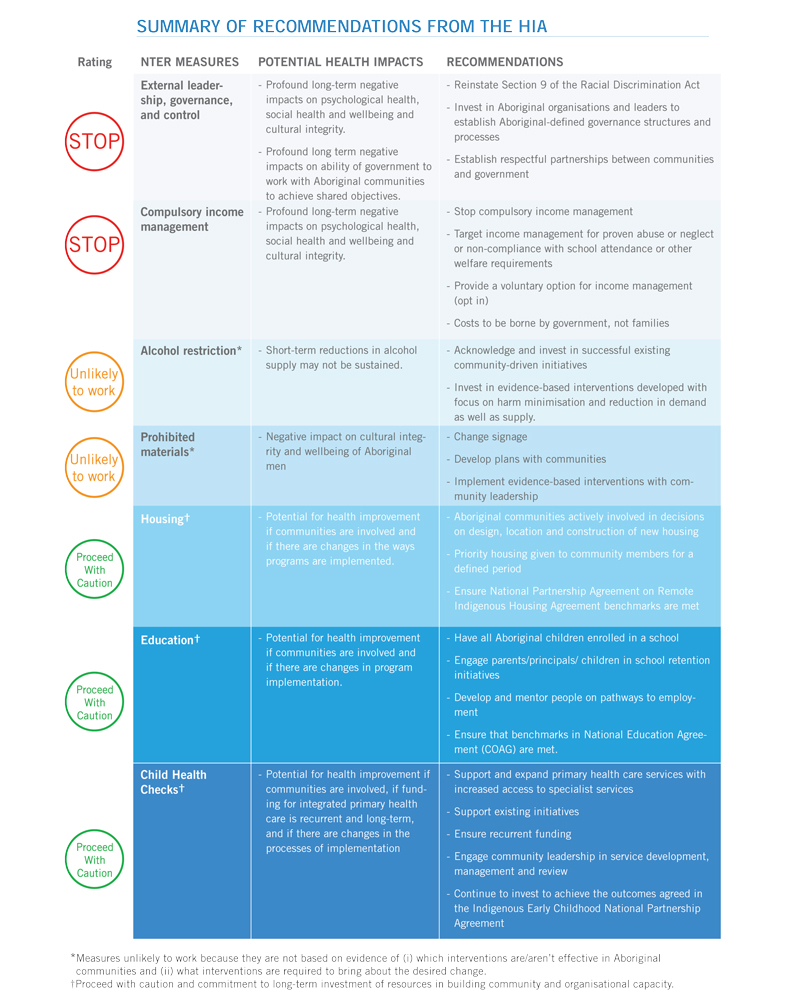
The Box summarises and rates the potential health impacts of the NTER measures, and outlines the recommendations of the health impact assessment (HIA) report.5
The health impact assessment of the NTER can be viewed online at http://www.aida.org.au/hia.aspx.
- 1. Wild R, Anderson P. Ampe akelyernemane meke mekarle “Little children are sacred”: report of the Northern Territory Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse. Darwin: Northern Territory Government, 2007.
- 2. Australian Government Department of Families, Housing, Community Services and Indigenous Affairs. About the Northern Territory Emergency Response. http://fahcsia.gov.au/sa/indigenous/progserv/ntresponse/about_response/overview/Pages/about_nter.aspx (accessed Apr 2010).
- 3. Australian Government Department of Families, Housing, Community Services and Indigenous Affairs. Communities and prescribed areas. http://www.fahcsia.gov.au/sa/indigenous/progserv/ntresponse/about_response/overview/communitiesprescribed/Pages/default.aspx (accessed Apr 2010).
- 4. World Health Organization European Centre for Health Policy. Health impact assessment: main concepts and suggested approach. Gothenburg consensus paper. Brussels: WHO, 1999. http://www.euro.who.int/document/PAE/Gothenburgpaper.pdf (accessed Apr 2010).
- 5. Australian Indigenous Doctors’ Association; Centre for Health Equity Training, Research and Evaluation, UNSW. Health impact assessment of the Northern Territory Emergency Response. Canberra: AIDA, 2010. http://www.aida.org.au/hia.aspx (accessed Apr 2010).
- 6. BasicsCard. http://www.centrelink.gov.au/internet/int (accessed Apr 2010).
AIDA would like to acknowledge the Health Impact Assessment Steering Committee, the Centre for Health Equity Training, Research and Evaluation at the University of New South Wales, the Fred Hollows Foundation, Professor Helen Milroy, and our community partners, key stakeholder interviewees and expert reviewers for their contribution to the report.