




The World Youth Day (WYD) Catholic youth festival was set up by Pope John Paul II in 1986. It is held in a different location every 2–3 years, and attracts large crowds of local and international pilgrims, particularly for the final Papal Mass (Box 1).1
WYD 2008, held in Sydney over 6 days (15–20 July), was anticipated to increase demand on Sydney hospitals, with implications for planning and resource allocation. There were 223 000 registered pilgrims, 110 000 of whom were visitors from 170 countries.2 There were 400 000 people at the Final Mass, and 500 000 attended the Papal “boat-a-cade” and motorcade.2
There have been no published studies on the impact of WYD events on hospitals, although prehospital care3 and systems for syndromic surveillance4 have been examined. Compared with other pilgrimages, WYD is unusual in that the pilgrimage is not to a holy site, as with the Hajj, whose health implications (eg, heatstroke, infection) have been well described.5,6 Instead, the festival is held in different cities, and the religious significance is largely in the Papal visit. Further, it is targeted to youth, which may affect the types of presentations.
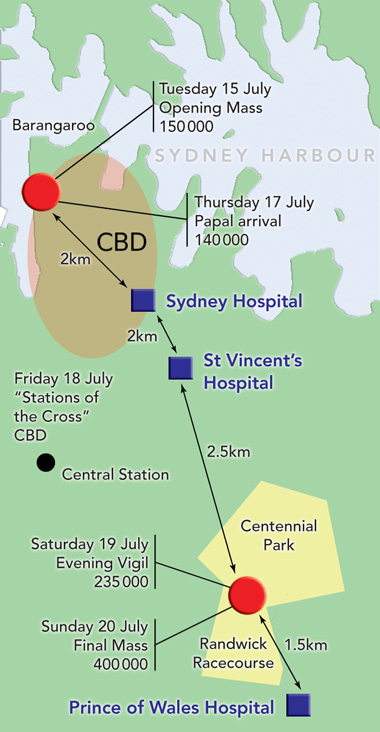
NSW Health public health surveillance provided a unique opportunity to describe the patterns of illness and presentation of WYD pilgrims. Most WYD 2008 events occurred within the inner city of Sydney (Box 2), which is mainly served by Sydney Hospital and St Vincent’s Hospital. We examined the impact of pilgrim presentations on these hospitals’ emergency departments (EDs), and any extra hospital workload associated with the event.
The resulting dataset was analysed and compared with the background ED caseload. Non-identifiable data from medical records of each presentation were examined and coded by presenting complaint and final diagnosis. Other variables examined were age, sex, country of birth, Australian residency, severity as measured by the Australasian Triage Scale (ATS; category 1 = immediately life-threatening; 2 = imminently life-threatening or important time-critical treatment; 3 = potentially life-threatening or situational urgency; 4 = potentially serious, situational urgency or significant complexity or severity; and 5 = less urgent or clinicoadministrative),7 and whether admitted to hospital.
There were 191 ED presentations by pilgrims during the study period — 87 to St Vincent’s Hospital and 104 to Sydney Hospital. Of these, 154 were during the period of official WYD events (Box 3), with a peak (19.3% of ED visits that day; 33/171) on 17 July, the date of the Papal arrival. Pilgrim presentations made up 7.8% (191/2445) of visits to these EDs for the period.
The most common problems were lower limb strain or sprain, infections, and asthma (Box 4). Upper respiratory tract infections and gastroenteritis were the most common infective problems. Although drug and alcohol presentations and acute psychiatric presentations are usually very common at these two EDs, these presentations were uncommon among pilgrims. There were two acute psychotic presentations and two cases of alcohol intoxication, compared with 29 psychotic episodes and 73 cases of alcohol intoxication from non-pilgrim patients in the same period (P = 0.019)
Pilgrims were less likely to require admission than other patients (45/191; 23.6% v 36.4%; P < 0.001). Admitted pilgrims had similar demographic characteristics to non-admitted pilgrims, but were more likely to have been triaged as higher severity. Australian pilgrims were more likely to be admitted to hospital than pilgrims from overseas (35.3% v 17.1%; P = 0.007). There was no single diagnosis, or group of diagnoses, particular to admitted pilgrims (Box 4).
Our study focused on the impact on EDs and hospitals, and is therefore limited in applicability to those settings. Although prehospital data were not analysed, prehospital presentations requiring transport to hospital from the inner-city area were captured. We did not capture data from presentations to other Sydney hospitals or outer metropolitan hospitals. As such, the primary outcome examined was the impact of the main events and tourist pilgrims in inner and eastern Sydney (Box 2). The hospital on the other side of the site of the Final Mass received 68 pilgrim attendances of similarly low acuity during the study period (Barbara Daly, ED Nursing Manager, Prince of Wales Hospital, personal communication, 2008).
Pilgrim presentations were less acute, and less often required admission compared with the other patients, as seen in previous research.8 As expected, many visits were due to falls and other injuries, flu-like illnesses and gastroenteritis, reflecting existing data on Australian mass gatherings.9 A sizeable minority of medical problems were exacerbations of chronic diseases, such as asthma. This reflects the experience in other pilgrimages, in particular with diseases requiring good ongoing management, which may be disturbed by travel and a new environment.10
Most pilgrims were young, in keeping with the theme of the event and in contrast to other types of Papal visits, which may be attended by older pilgrims.11 This may partly account for the low acuity and burden of disease observed.
Pilgrims were more often women, while the normal caseload of the two EDs has a higher proportion of men than women. As there were no epidemiological differences between these men and women, this probably reflects the profile of registered pilgrims with a female-to-male ratio of 1.25 : 1 (Katrina Lee, Director of Catholic Communications and Broadcast Manager, WYD 2008, personal communication, 2008). A study of Australian pilgrims to the previous WYD (2005) under the age of 18 years found that 65% of those surveyed were female.12
Compared with the well described effects of the heat in mass gatherings11,13,14 and the Hajj pilgrimage, the cold was the environmental factor anticipated in this event.15 Taking place in winter, air temperature throughout the event was seasonably low, with minimal rain. Notably, many thousands of pilgrims attended an overnight vigil before the Final Mass, sleeping outside in the open while air temperature dropped to 8.6°C. Despite this, there were no admissions for exposure or hypothermia. A message about the need to stay warm overnight had been stressed by the Ambulance Service of NSW and NSW Health.15
Analysis of mass gatherings in Australia generated a range of predicted hospital attendance of 0.01 to 0.55 per 1000 event participants.9 We uniquely describe a multiday complex mass gathering with more variables than a sporting event16,17or a rock concert.18 By dividing the presentations recorded in this study by the overall attendance given by the event coordination body, there was an attendance rate of about 0.05 per 1000 event participants per day for the inner-city hospitals studied (although this does not account for pilgrims who may have been treated at other hospitals). This confirms that WYD lies in the lower range, and as such has a lower impact on hospitals. Our study, which also analysed hospital admissions, documented the low burden on hospitals, whereas most existing literature reports aggregated prehospital presentations in a variety of health care settings.
- Myles W H Smith1
- Gordian W O Fulde2
- Patricia M Hendry2
- 1 St Vincent’s Clinical School, University of New South Wales, Sydney, NSW.
- 2 Emergency Department, St Vincent’s Hospital, Sydney, NSW.
None identified.
- 1. WYD 2008. History of WYD. Updated 21 Jul 2008. http://www.wyd2008.org/index.php/en/about_wyd08/history (accessed Aug 2008).
- 2. WYD 2008. Final statistics. Updated 21 Jul 2008. http://www.wyd2008.org/index.php/en/about_wyd08/final_statistics (accessed Aug 2008).
- 3. Lukins JL, Feldman MJ, Summers JA, Verbeek PR. A paramedic-staffed medical rehydration unit at a mass gathering. Prehosp Emerg Care 2004; 8: 411-416.
- 4. Bassil KL, Henry B, Rea E, et al. Public health surveillance for World Youth Day. Toronto, Canada, 2002. Morb Mortal Wkly Rep 2005; 54 Suppl: 183.
- 5. Al-Ghamdi SM, Akbar HO, Qari YA, et al. Pattern of admission to hospitals during Muslim pilgrimage (Hajj). Saudi Med J 2003; 24: 1073-1076.
- 6. Ahmed QA, Arabi YM, Memish ZA. Health risks at the Hajj. Lancet 2006; 367: 1008-1015.
- 7. Australasian College for Emergency Medicine. Guidelines on the implementation of the Australasian Triage Scale in emergency departments. Melbourne: ACEM, 2000. http://www.acem.org.au/media/policies_and_guidelines/G24_Implementation__ATS.pdf (accessed Aug 2008).
- 8. Varon J, Fromm RE, Chanin K, et al. Critical illness at mass gatherings is uncommon. J Emerg Med 2003; 25: 409-413.
- 9. Arbon P. Planning medical coverage for mass-gatherings in Australia: what we currently know. J Emerg Nurs 2005; 31: 346-350.
- 10. Beshyah SA, Sherif IH. Care for people with diabetes during the Moslem pilgrimage (Haj): an overview. Libyan J Med 2008; 3: 26-30.
- 11. Milsten AM, Maguire BJ, Bissell RA, Seaman KG. Mass-gathering medical care: a review of the literature. Prehospital Disaster Med 2002; 17: 151-162.
- 12. Rymarz R. Who goes to World Youth Day? Some data on under-18 Australian participants. J Beliefs Values 2007; 28: 33-43.
- 13. Dolney TJ, Sheridan SC. The relationship between extreme heat and ambulance response calls for the city of Toronto, Ontario, Canada. Environ Res 2006; 101: 94-103.
- 14. Milsten AM, Seaman KG, Liu P, et al. Variables influencing medical usage rates, injury patterns, and levels of care for mass gatherings. Prehospital Disaster Med 2003; 18: 334-346.
- 15. Park N. Pilgrims told to rug up for sleepout. The Australian 2008; 19 Jul. http://www.news.com.au/story/0,23599,24044138-5016937,00.html (accessed Nov 2008).
- 16. Wassertheil J, Keane G, Fisher N, Leditschke J. Cardiac arrest outcomes at the Melbourne Cricket Ground and Shrine of Remembrance using a tiered response strategy: a forerunner to public access defibrillation. Resuscitation 2000; 44: 97-104.
- 17. Dutch MJ, Senini LM, Taylor DJ. Mass gathering medicine: the Melbourne 2006 Commonwealth Games experience. Emerg Med Australas 2008; 20: 228-233.
- 18. Fulde GW, Forster SL, Preisz P. Open air rock concert: an organised disaster. Med J Aust 1992; 157: 820-822.
Abstract
Objective: To characterise the nature and impact of World Youth Day (WYD) 2008 on emergency department (ED) presentations at key hospitals.
Design, setting and participants: Retrospective analysis of WYD pilgrims presenting to the EDs of St Vincent’s Hospital and Sydney Hospital, 9–23 July 2008.
Main outcome measures: Frequency of pilgrim ED presentations; presenting complaint, Australasian Triage Scale category, diagnosis, admission to hospital and demographic characteristics.
Results: 191 pilgrims presented at the two EDs during the study period, comprising 7.8% of all visits to these EDs. Pilgrims had a median age of 22 years, and most were international visitors. The female-to-male ratio was 1.7 : 1. The most common diagnoses were lower limb strain or sprain, infections, and acute asthma. Pilgrims presented with less severe illnesses (with lower triage scores), and were less likely to be admitted to hospital than other patients.
Conclusions: The pilgrim caseload was small, and these presentations were less acute and less likely to result in admission than non-pilgrim presentations. Thus, the overall impact on the hospitals was very small.