




Research into hospital doctors’ work has largely focused on the hours they work,1-3 rather than on what they do. A review of MEDLINE revealed few quantitative data describing how hospital doctors actually spend their time. Few hospitals know, for example, how much time their doctors spend in critical areas, such as direct patient care, versus searching for missing records.
Obtaining baseline data about current patterns of work is important for assessing the effects of interventions designed to improve care delivery models. A good example is the increased investment in and implementation of computerised clinical information systems, which are expected to improve the safety and efficiency of health care delivery.4 While such systems are promoted as reducing administrative tasks of clinicians,5 concerns have been raised that many tasks, such as ordering medication and tests, may take longer with new systems than paper-based systems.6,7 Further, introducing new systems may change communication patterns, with doctors spending more time alone,7 and less time in face-to-face communication with nurses.8,9 Without data reflecting current task time distributions, the accuracy of such claims cannot be tested, nor can we measure the extent to which any time costs are offset by safety gains.10
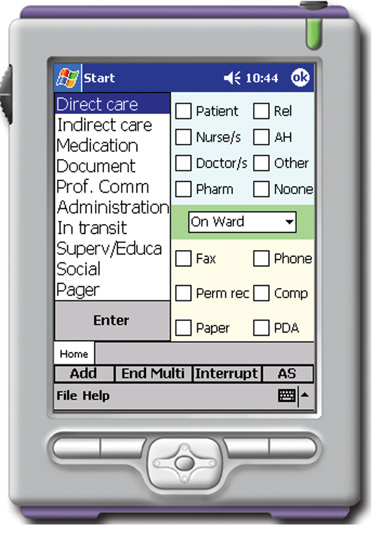
A multidimensional work task classification system was designed and incorporated into a handheld computer (a personal digital assistant).10,11 Pilot testing occurred at the study site, with 7 hours’ observation and review by seven doctors. On the basis of feedback, three subtask categories were added — searching for x-rays, searching for missing medical records and writing discharge summaries — which doctors reported consumed “all our time” or “wasted” their time. A category to identify interruptions by a pager was also added.
The interface design included 10 broad mutually exclusive work categories (Box 1). Some categories had drop-down menus for greater detail (Box 2). Each task was automatically time-stamped. For each task, the data collector recorded whom the doctor was with, information tools used in the task, whether the doctor was on or off his or her allocated ward and officially on or off duty (eg, continuing or completing tasks after a designated shift end).
For all groups, professional communication consumed the greatest proportion of time (Box 3). Registrars spent proportionally more time in professional communication, and in supervision and education than either residents or interns (χ2 = 145.5; P < 0.001). On average, interns spent less time in direct care and considerably more time completing documentation and in general administrative tasks (χ2 = 599.7; P < 0.001). The proportion of observed time interns spent documenting (22%) was almost double that engaged in direct care.
For all groups, most work was undertaken with another person, most often another doctor (Box 4). On average, nearly a quarter of tasks were performed alone. Registrars undertook a significantly smaller percentage of work alone than the other doctors (χ2 = 38.7; P < 0.001). Fifteen per cent of tasks were undertaken with a patient. These tasks consumed an average of 21% of doctors’ time. Most work tasks (75.1%) were completed in the doctor’s allocated ward, with registrars less likely to do this (70.2%) than interns (76.0%) and residents (77.6%; χ2 = 29.85; P < 0.001). Two per cent of tasks were identified as occurring while the doctor was not officially on duty.
Hospital doctors spent two-thirds of their time on three broad categories of tasks: professional communication, social activities and indirect care. The work of interns differed significantly from that of residents and registrars and was characterised by considerably more time spent in documentation and administrative activities, and less on direct care. This is consistent with reports of interns’ dissatisfaction with the high level of indirect care and administrative tasks they are required to undertake.12,13
Over half of these doctors’ work was carried out in the presence of another doctor and about a quarter was undertaken alone. On average, doctors spent more time with patients than they did with nurses or any other non-medical health professional. The rate of interruptions to these ward doctors (2.9 per hour) was less than half of the reported rates for doctors in emergency departments (6 to 15 per hour).14-18
We observed doctors only in the wards during weekdays from 08:30 until 19:00, so results may not be generalisable to weekends, evenings or early morning shifts. Direct, close observation lends itself to the Hawthorne effect, whereby participants improve their performance while being observed. In this study, the effect might be expected for time spent in social activities. Yet social activities were observed to take more time than most of the other types of task. We did not have the power to examine differences between wards, but have previously found few differences between nurses’ patterns of work across wards, despite beliefs that these existed before measurement.10
The study represents one of the few, and largest, time and motion studies of hospital doctors identified, and as such, provides a useful baseline for future studies. Our results support previous survey data of junior doctors’ experiences,1,12 and debunk commonly held perceptions about the time consumed by specific tasks. For example, doctors had asked us to measure the time spent searching for x-rays and records, because these tasks occupied “all of our time”. Yet they consumed less than 1% of their time. The greater weight given to these tasks in discussions clearly reflects the frustration these tasks generate. We have reported a similar situation among nurses, who complained of time wasted following up illegible medication orders, yet when this was measured, we found nurses spent, on average, less than 2 minutes per shift on this task.19
2 Work tasks, subtasks and associated definitions
4 Percentage of all work tasks (n = 6243) performed by doctors alone or with other people, and percentage undertaken using specific information tools*
* Percentages do not add to 100 as some tasks were undertaken at the same time (ie, when doctors were multitasking). † A permanent record (as on the list in Box 2) is a part of the patient’s medical record. |
|||||||||||||||
Received 8 July 2007, accepted 16 December 2007
- Johanna I Westbrook1
- Amanda Ampt2
- Leanne Kearney3
- Marilyn I Rob4
- Health Informatics Research and Evaluation Unit, University of Sydney, Sydney, NSW.
This research was funded by an Australian Research Council Linkage Grant in partnership with the Health Department of New South Wales (LP0347042). Johanna Westbrook is supported by a National Health and Medical Research Council fellowship (300567). The authors had full independence from the funding bodies.
None identified.
- 1. Turnbull J, Miles N, Gallen I. Junior doctors’ on call activities: differences in workload and work patterns among grades. BMJ 1990; 301: 1191-1192.
- 2. Scallon S. Education and the working patterns of junior doctors in the UK: a review of the literature. Med Educ 2003; 37: 907-912.
- 3. Kapur N, House A. Working patterns and the quality of training of medical house officers: evaluating the effect of the ‘new deal’. Med Educ 1998; 32: 432-438.
- 4. Deloitte. Queensland Health eHealth Strategy. Brisbane: Queensland, 2006. http://www.health.qld.gov.au/ehealth/eh_strat_public.pdf (accessed Jan 2008).
- 5. HealthSmart. Clinical systems. Melbourne: Victorian Government Department of Human Services, 2007. http://www.health.vic.gov.au/healthsmart/clinsys.htm (accessed Jan 2008).
- 6. Poissant L, Pereira J, Tamblyn R, et al. The impact of electronic health records on time efficiency of physicians and nurses: a systematic review. J Am Med Inform Assoc 2005; 12: 505-516.
- 7. Shu K, Boyle D, Spurr C, et al. Comparison of time spent writing orders on paper with computerized physician order entry. Medinfo 2001; 10 (Pt 2): 1207-1211.
- 8. Beuscart-Zephir M, Pelayo S, Anceaux F, et al. Impact of CPOE on doctor-nurse cooperation for the medication ordering and administration process. Int J Med Inform 2005; 74: 629-641.
- 9. Carpenter JD, Gorman PN. What’s so special about medications: a pharmacist’s observations from the POE study. Proc AMIA Symp 2001; 95-99.
- 10. Westbrook J, Ampt A, Williamson M, et al. Methods for measuring the impact of health information technologies on clinicians' patterns of work and communication. Medinfo 2007; 12: 1083-1087.
- 11. Ampt A, Westbrook J, Creswick N, et al. Comparison of self-reported and observational work sampling techniques to measure nurses’ work. J Health Serv Res Policy 2007; 12: 18-24.
- 12. Rolfe I, Pearson S, Sanson-Fisher R, et al. Measuring the hospital experiences of junior doctors. Med Educ 1998; 32: 312-319.
- 13. Dally P, Ewan C, Pitney W. Assessment of an Australian medical internship. Med Educ 1984; 18: 181-186.
- 14. Coiera E, Jayasuriya R, Hardy J, et al. Communication loads on clinicians in the emergency department. Med J Aust 2002; 176: 415-418. <MJA full text>
- 15. Chisholm C, Collison K, Nelson D, et al. Emergency department workplace interruptions: are emergency physicians “interrupt-driven” and “multitasking”? Acad Emerg Med 2000; 7: 1239-1243.
- 16. France D, Levin S, Hemphill R, et al. Emergency physicians’ behaviours and workload in the presence of an electronic whiteboard. Int J Med Inform 2005; 74: 827-837.
- 17. Laxmisan A, Hakimzada F, Sayan OR, et al. The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform 2007; 76: 801-811.
- 18. Fairbanks R, Bisantz A, Summ M. Emergency department communication links and patterns. Ann Emerg Med 2007; 50: 396-406.
- 19. Ampt A, Westbrook J. Measuring nurses’ time in medication related tasks before the implementation of an electronic medication management system. In: Westbrook J, Coiera E, Callen J, Aarts J, eds. Information technology in health care. 3rd International Conference on Technology in Health Care: socio-technical approaches. Studies in health technology and informatics. Vol. 130. Sydney. IOS Press, 2007: 157-168.
Abstract
Objective: To quantify time doctors in hospital wards spend on specific work tasks, and with health professionals and patients.
Design: Observational time and motion study.
Setting: 400-bed teaching hospital in Sydney.
Participants: 19 doctors (seven registrars, five residents, seven interns) in four wards were observed between 08:30 and 19:00 for a total of 151 hours between July and December 2006.
Main outcome measures: Proportions of time in categories of work; proportions of tasks performed with health professionals and patients; proportions of tasks using specific information tools; rates of multitasking and interruptions.
Results: The greatest proportions of doctors’ time were in professional communication (33%; 95% CI, 29%–38%); social activities, such as non-work communication and meal breaks (17%; 95% CI, 13%–21%), and indirect care, such as planning care (17%; 95% CI, 15%–19%). Multitasking involved 20% of time, and on average, doctors were interrupted every 21 minutes. Most tasks were completed with another doctor (56%; 95% CI, 55%–57%), while 24% (95% CI, 23%–25%) were undertaken alone and 15% (95% CI, 15%–16%) with a patient. Interns spent more time completing documentation and administrative tasks, and less time in direct care than residents and registrars. The time interns spent documenting (22%) was almost double the time they were engaged in direct patient care.
Conclusions: Two-thirds of doctors’ time was consumed by three work categories: professional communication, social activities and indirect care. Doctors on wards are interrupted at considerably lower rates than those in emergency and intensive care units. The results confirm interns’ previously reported dissatisfaction with their level of administrative work and documentation.