




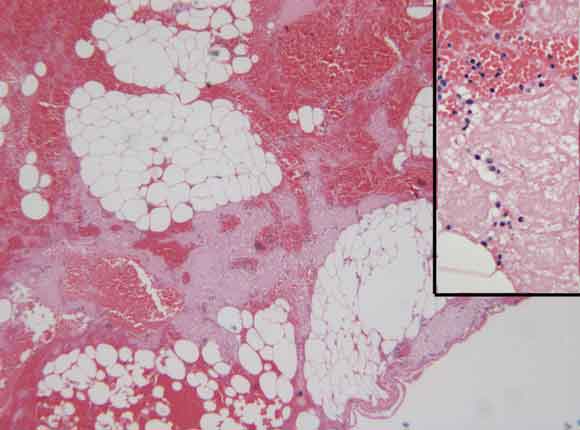
A 44-year-old woman presented with a 3-day history of worsening right upper quadrant pain associated with nausea, anorexia and fever. She had localised tenderness and guarding in the epigastrium. Initial ultrasound imaging showed a distended gallbladder containing calculi, without wall thickening. A computed tomography scan (performed because of increasing pain) showed a whorled structure in the anterior abdomen (Box 1). At laparotomy this was seen to be torsion of a segment of the greater omentum. Histology of the resected specimen showed congestion of the vessels, haemorrhagic infarction and focal fat necrosis (Box 2). She made an uncomplicated and rapid recovery.
Primary omental torsion is a rare cause of acute abdomen. It may affect children and adults, and is commonly misdiagnosed preoperatively as appendicitis. Some cases have presented as acute cholecystitis.1,2 Kimber et al identified 13 cases of omental torsion or infarction in about 8000 cases of suspected appendicitis over a 20-year period.3
Large meals, sudden postural change, and abdominal trauma may be precipitating factors in primary torsion,4 while adhesions, hernia, tumour or focus of inflammation3 occur with secondary torsion. Resection is the preferred treatment,3,4 although some clinicians suggest conservative management2 when the diagnosis is apparent on computed tomography. Laparoscopic resection has also been advocated.5

- Wen-Chan Yeow1
- Mohan V Jayasundera2
- Graham Hool3
- Rajalingam Sinniah4
- Royal Perth Hospital, Perth, WA.
- 1. Saborido BP, Romero CJ, Medina EM, et al. Idiopathic segmental infarction of the greater omentum as a cause of acute abdomen: report of two cases and review of the literature. Hepatogastroenterology 2001; 48: 737-740.
- 2. Abadir JS, Cohen AJ, Wilson SE. Accurate diagnosis of infarction of omentum and appendices epiploicae by computed tomography. Am Surg 2004; 70: 854-857.
- 3. Kimber CP, Westmore P, Hutson JM, et al. Primary omental torsion in children. J Paediatr Child Health 1996; 32: 22-24.
- 4. Itinteang T, van Gelderen WF, Irwin RJ. Omental whirl: torsion of the greater omentum. ANZ J Surg 2004; 74: 702-703.
- 5. Sanchez J, Rosado R, Ramirez D, et al. Torsion of the greater omentum: treatment by laparoscopy. Surg Laparosc Endosc Percutan Tech 2002; 12: 443-445.