




An 80-year-old woman with a history of hypertension presented to the emergency department with a 3-hour history of dyspnoea and precordial discomfort. Serum concentrations of troponin T, creatine kinase and creatine kinase MB isoenzyme were normal. An electrocardiogram (Box 1) showed changes consistent with myocardial ischaemia. When the patient developed haemodynamic instability, cardiac catheterisation was performed (Box 2). The patient’s condition improved after an intra-aortic balloon pump (a catheter-mounted balloon positioned in the descending aorta and timed to inflate during diastole) was placed for the management of cardiogenic shock. An echocardiogram 3 weeks later showed normal left ventricular size and function.
The patient had acute transient apical ballooning with normal coronary arteries (“Takotsubo” cardiomyopathy). First described in 1990,1 the presentation is similar to that of acute transmural myocardial ischaemia, with chest symptoms and electrocardiographic changes ranging from ST-segment elevation to T-wave inversion without ST shifts.2,3 Postulated triggering factors for transient apical ballooning have included onset or exacerbation of systemic disorders (eg, cerebrovascular accident, asthma, acute abdomen) and extreme emotional distress.2 Women are 6–12 times more likely to be affected than men.2-4 The in-hospital mortality rate is less than 1%,2 and there is usually complete functional recovery of the left ventricle within 2 weeks.3,4 The 2-year recurrence rate is less than 3%.2 The optimal therapy for this condition is unknown.
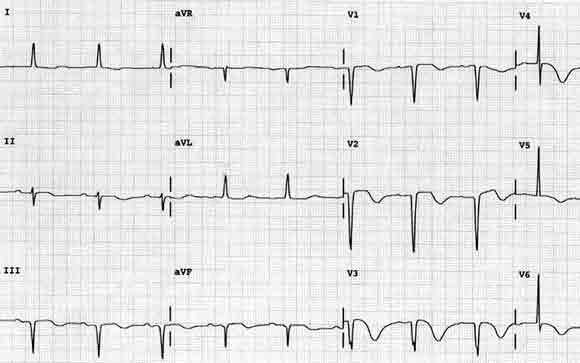
1 Electrocardiogram, showing delayed R-wave progression and inverted T waves in the anterolateral leads
2 Images from cardiac catheterisation
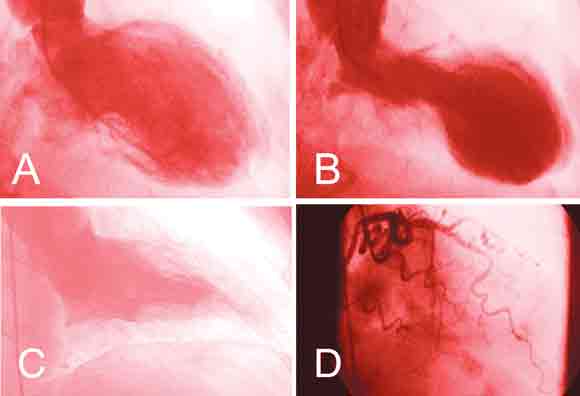
A. End-diastolic left ventriculogram.
B. End-systolic left ventriculogram, showing akinesia/dyskinesia of the apical and mid portions of the left ventricle and hyperdynamic motion at the base. The left ventricular ejection fraction was 30%, with elevated left ventricular end-diastolic pressure of 35 mmHg.
C. Normal end-systolic left ventriculogram (from a different patient).
D. Left coronary angiogram, showing a normal left anterior descending artery.
- Constantin B Marcu1
- Kristen M Andresen2
- Thomas J Donohue3
- Section of Cardiology, Hospital of Saint Raphael, Yale University School of Medicine, New Haven, CT, USA.
- 1. Satoh H, Tateishi H, Uchida T, et al. Takotsubo-type cardiomyopathy due to multivessel spasm. In: Kodama K, Haze K, Hon M, editors. Clinical aspects of myocardial injury: from ischemia to heart failure [in Japanese]. Tokyo: Kagakuyouronsya Co., 1990: 56-64.
- 2. Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol 2001; 38: 11-18.
- 3. Abe Y, Kondo M, Matsuoka R, et al. Assessment of clinical features in transient left ventricular apical ballooning. J Am Coll Cardiol 2003; 41: 737-742.
- 4. Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart 2003; 89: 1027-1031.