




The small intestine remains difficult to investigate with available technology. Push enteroscopy allows examination of only up to 80–120 cm beyond the ligament of Treitz,1 while intraoperative enteroscopy involves a general anaesthetic and laparotomy. Barium follow-through and enteroclysis (double contrast small-bowel follow-through) allows indirect examination of the small bowel, but has a low yield, especially in detecting flat pathological lesions such as vascular malformations.2 Capsule endoscopy provides an alternative to overcome the limitations of these methods.
The use of the capsule in 10 normal human volunteers was first described in May 2000.3 Since then, more than 8000 capsule examinations have been performed.4 We report our initial experience of capsule endoscopy at a major referral hospital.
Subjects were 60 consecutive patients who underwent capsule endoscopy at St Vincent's Hospital, Melbourne, Victoria, between 4 July 2001 and 8 September 2002. The first 20 patients were recruited as part of a trial comparing capsule endoscopy and enteroscopy in patients with obscure gastrointestinal bleeding (OGB).5 Subsequently, all patients undergoing capsule endoscopy at our hospital for various indications, including OGB and suspected Crohn's disease of the small bowel, were included in the study.
By definition, all patients with OGB had no abnormalities found on complete gastroscopy and colonoscopy.
Patients with suspected small-bowel Crohn's disease may or may not have had a previous diagnosis of Crohn's disease. The suspicion was based on a combination of clinical features, including pain, diarrhoea and weight loss, raised levels of inflammatory markers and abnormal radiological or endoscopic findings. These patients were required to have a prior small-bowel barium study to exclude strictures.
All patients referred for investigation of the small bowel were assessed for eligibility. Exclusion criteria included a cardiac pacemaker, pregnancy, dysphagia and known small-bowel strictures. Patients fasted from midnight, and in the morning swallowed the capsule endoscope with a glass of water mixed with simethicone (1 mL), which helps eradicate small bubbles in the small bowel. After 8 hours, patients returned to have the recording equipment removed.
Capsule images were reviewed by two gastroenterologists, and questionable findings were discussed. Positive findings were defined as detected abnormalities that were potentially related to the presenting problem. We considered blood seen in isolation in the small bowel as a positive finding. Blood alone is not a diagnosis, but may be helpful in localising the source and support the use of more invasive procedures such as intraoperative enteroscopy.
This study was approved by the St Vincent's Hospital Research Ethics Committee.
Sixty patients underwent 61 capsule endoscopy procedures. Thirty-six patients (60%) were men. The age range was 17–86 years (mean, 56.1 years). The indications and findings in these patients are shown in Box 1.
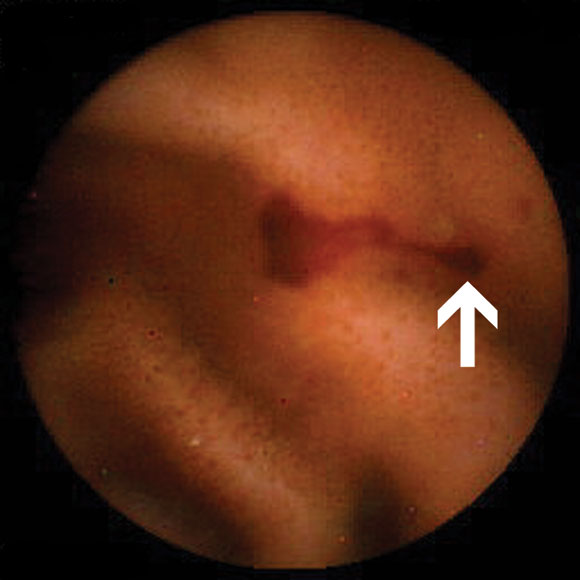
In 47 patients with OGB, abnormal findings (Box 2A) were detected in 32 (68%). Four had abnormalities detected in the stomach, and one in the caecum. Eight had abnormalities judged to be within reach of push enteroscopy. Eighteen of the 47 (38%) patients had a change in management as a result of capsule endoscopy (Box 3).
In one patient referred with OGB and abdominal pain, the capsule was not excreted. This was confirmed on an abdominal x-ray and computed tomo-graphy scan of the abdomen. At laparo-tomy, the capsule was found to be proximal to an ileal stricture, and a small-bowel resection was performed. Histological results were consistent with Crohn's disease.
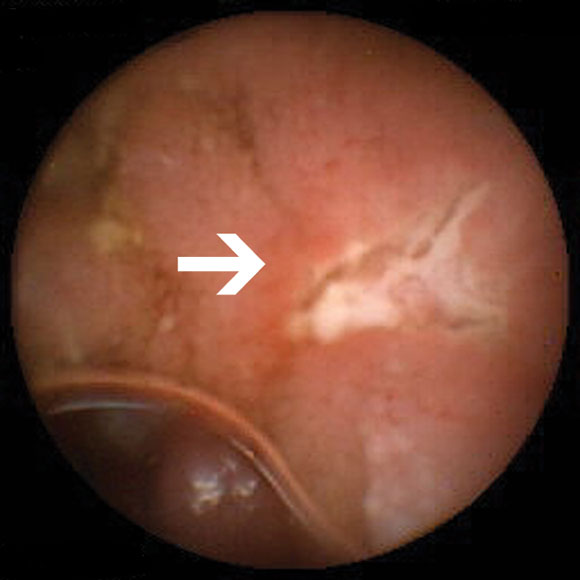
Of the nine patients referred for investigation of small-bowel Crohn's disease, none had been taking non-steroidal anti-inflammatory drugs (NSAIDs) before onset of their symptoms. Small-bowel erosions or ulcers (Box 2B) were seen in seven of these nine patients. Enteroclysis demonstrated mucosal irregularity in two of the seven patients with abnormal findings on capsule endoscopy. Management was changed in five of the nine patients. One patient was lost to follow-up. Changes in management are summarised in Box 4.
Four patients were referred for other indications (Box 1). No abnormality was seen in the patient with hereditary non-polyposis colorectal cancer (HNPCC), but the examination was incomplete. A subsequent laparotomy revealed an adenocarcinoma in the distal small bowel. A patient with Peutz–Jeghers syndrome had multiple small polyps and erosions in the ileum. Her management was changed in that surgery was deferred.
In our cohort, OGB was the main indication for referral for capsule endoscopy. For investigating OGB, this technique has been reported to have a greater yield than push enteroscopy;6-9 this is similar to our experience.2 In addition, although the reported yield for push enteroscopy in OGB is 38%–75%, the true yield is lower because many of these findings (28%–75%) are within reach of an endoscope.10 Therefore, a repeat endoscopy is justifiable in OGB. However, push enteroscopy is still useful for biopsy and applying local therapy beyond the reach of a normal endoscope. A repeat colonoscopy is also appropriate in OGB, as lesions may be missed on the first colonoscopy,10 especially if the bowel preparation was suboptimal. Hence, we suggest repeating upper and lower endoscopies before capsule endoscopy. We propose an algorithm for investigating OGB in Box 5.
Capsule endoscopy has been reported to have a greater yield than small-bowel barium follow-through in evaluation of small-bowel disease.11 Our experience is similar. In our initial 20 patients with OGB, none had positive findings on barium studies. This included six patients with arteriovenous malformations, one with a gastrointestinal stromal tumour in the duodenum and another with an ileal stricture and erosions. Despite their low yield,10 small-bowel barium studies are still useful in ruling out significant strictures in some patients with suspected small-bowel Crohn's disease, symptoms suggestive of small-bowel obstruction and a history of prolonged NSAID use prior to capsule endoscopy. NSAIDs may cause "diaphragm-like" strictures that impede passage of the capsule.12
In suspected Crohn's disease of the small bowel, our results are similar to other studies. These have reported an increased yield in detecting erosions and ulcers missed by conventional investigations, including ileoscopy and small-bowel barium studies.4,13 Our findings led to a change in management in five out of seven patients followed up (Box 4). We believe that capsule endo-scopy is useful in two distinct situations. First, in investigating patients with suspected de novo small-bowel Crohn's disease based on specific criteria, including abdominal pain, fever, weight loss, anaemia, elevated erythrocyte sedimentation rate but negative results on conventional investigations.4 Second, in patients whose clinical and laboratory findings are out of keeping with the known extent and severity of disease using conventional investigations.
Although we have investigated only two patients with pain as a predominant symptom, we suspect that the yield will be low in this group unless there are other clinical features and investigations suggestive of organic pathology.
All the capsules in this study used the original version of the battery. Improvements in the battery life and power consumption of the capsule are expected to increase the proportion of completed small-bowel studies.
One of our patients (1.7%) had a prolonged retention of the capsule. In initial clinical trials by Given Imaging, seven out of 973 patients (0.75%) had a prolonged retention of the capsule needing intervention to remove the capsule (Warren Bingham, Vice President, Given Imaging, Australia, personal communication). Currently, we recommend that patients have an abdominal x-ray 2 weeks after the investigation if they have not observed the capsule pass within that time.
The major limitation of our study and other studies is the lack of a gold standard, such as intraoperative enteroscopy, to determine accuracy, sensitivity and specificity. Terms such as "diagnostic yield" and "positive findings" are crude measures, as the rates of false-positive and false-negative results are unknown. In addition, the clinical significance of a finding is sometimes difficult to ascertain. Examples include small non-bleeding arteriovenous malformations and submucosal masses. The significance of these findings and clinical outcomes will only become known with longer term follow-up.
Based on our initial experience, we believe capsule endoscopy is useful in investigating and guiding further management of patients with suspected small-bowel disease, especially OGB and suspected small-bowel Crohn's disease.
1: Findings in 60 patients who underwent capsule endoscopy
Obscure gastrointestinal bleeding (47 patients)
Occult bleeding (26 patients)*
4 small-bowel arteriovenous malformation
3 small-bowel blood alone
3 blood and small-bowel arteriovenous malformation
2 blood and small-bowel polyp
1 blood and gastric antral vascular ectasia
1 caecal arteriovenous malformation
1 gastric arteriovenous malformation
1 gastric ulcer
1 Cameron's erosions (linear erosions in a hiatus hernia at the site of diaphragmatic indentation)
1 flattened villi
8 negative findings
Overt bleeding (21 patients)
6 small-bowel arteriovenous malformation
3 blood and small-bowel arteriovenous malformation
2 blood alone
1 blood and small-bowel tumour
1 small-bowel Crohn's disease
1 small-bowel submucosal mass
7 negative findings
Total positive findings: 32/47 (68%)
Suspected small-bowel Crohn's disease (9 patients)
Known Crohn's disease (7 patients)
6 small-bowel ulcers or erosions
1 negative finding
Newly suspected Crohn's disease (2 patients)
1 small-bowel ulcers or erosions
1 negative finding
Total positive findings: 7/9 (78%)
Other indications (4 patients)
Abdominal pain with diarrhoea (1 patient) or loss of weight (1 patient)
2 negative findings
HPNCC (1 patient)
1 negative finding
PJS and abdominal pain (1 patient)
1 small polyps
Total positive findings: 1/4 (25%)
HPNCC = hereditary non-polyposis colon cancer. PJS = Peutz–Jeghers syndrome.
* Iron deficiency anaemia with or without positive faecal occult blood test.
3: Changes to management after capsule enteroscopy for patients with obscure gastrointestinal bleeding (OGB)
Overt bleeding (5 patients)
2 surgery and resection of bleeding source, no further OGB
1 repeat enteroscopies for treatment of proximal small-bowel arteriovenous malformation
1 normal on laparotomy (false positive)
1 surgery planned
Occult bleeding (13 patients)
4 enteroscopy for treatment of proximal small-bowel arteriovenous malformations
3 surgery for resection of small-bowel source of bleeding, no further OGB
1 repeat gastroscopy for treatment of gastric antral vascular ectasia
1 repeat colonoscopy for treatment for caecal arteriovenous malformation, no further OGB
1 normal on laparotomy (false positive)
1 surgery planned
1 planned laparotomy cancelled
1 proton pump inhibitor added
4: Changes to management after capsule endoscopy for patients with suspected small-bowel Crohn's disease
Clinical features |
Capsule findings |
Change to management |
|||||||||
Previously diagnosed Crohn's disease (7 patients) |
|||||||||||
Abdominal pain, diarrhoea, fever. Normal ileoscopy, irregular terminal ileum on enteroclysis |
Ileal ulcers |
Increased immunosuppression |
|||||||||
Abdominal pain, diarrhoea. Terminal ileitis |
Proximal small-bowel and ileal ulcers |
Increased immunosuppression |
|||||||||
Abdominal pain, diarrhoea. Ileoscopy failed |
Proximal small-bowel ulcers |
Lost to follow-up |
|||||||||
Abdominal pain, diarrhoea. Crohn's colitis, normal ileoscopy |
Normal small bowel |
No change — continued immunosuppression |
|||||||||
Abdominal pain, diarrhoea. Terminal ileitis, irregular terminal ileum on enteroclysis |
Ileal ulcers only |
No change — continued immunosuppression |
|||||||||
Abdominal pain, diarrhoea. Neoterminal ileal erosions |
Minimal neoterminal ileum erosions |
Cease immunosuppression |
|||||||||
Abdominal pain. Normal ileoscopy |
Minimal terminal ileum erosions |
Treated as irritable bowel syndrome |
|||||||||
Newly suspected Crohn's disease (2 patients) |
|||||||||||
Abdominal pain, diarrhoea. Macroscopically abnormal ileoscopy but normal histology |
Normal small bowel |
Ceased azathioprine |
|||||||||
Weight loss, diarrhoea. Macroscopically abnormal ileoscopy but normal histology |
Terminal ileal ulceration |
Patient declined follow-up |
|||||||||
Received 20 September 2002, accepted 3 April 2003
- André K H Chong1
- Andrew C F Taylor2
- Ashley M Miller3
- Paul V Desmond4
- Gastroenterology Department, St Vincent's Hospital, Fitzroy, VIC.
André Chong is supported by an NHMRC Medical Postgraduate Scholarship. The first 20 investigations in this study were sponsored by Given Imaging, Yoqneam, Israel.
None identified.
- 1. Lewis B. The history of enteroscopy. Gastrointest Endosc Clin North Am 1999; 9: 1-11.
- 2. Maglinte D, Kelvin F, O'Connor K, et al. Current status of small bowel radiography. Abdom Imaging 1996; 21: 247-257.
- 3. Iddan G, Meron G, Glukhovski A, et al. Medical engineering: wireless capsule endoscopy. Nature 2000; 405: 417.
- 4. Fireman Z, Mahajna E, Broide E, et al. Diagnosing small bowel Crohn's disease with wireless capsule endoscopy. Gut 2003; 52: 390-392.
- 5. Chong A, Miller A, Taylor A, et al. Prospective evaluation of push enteroscopy versus capsule endoscopy in patients with gastrointestinal bleeding of obscure origin [abstract]. J Gastroenterol Hepatol 2002; 17 Suppl: A131.
- 6. Pennazio M, Santucci R, Rondonotti E, et al. Wireless capsule endoscopy in patients with obscure gastrointestinal bleeding: results of the Italian multicentre experience [abstract]. Gastrointest Endosc 2002; 55: AB87.
- 7. Delvaux M, Saurin J, Gaudin J, et al. Comparison of wireless endoscopic capsule and push-enteroscopy in patients with obscure occult/overt digestive bleeding: results of a prospective, blinded, multicentre trial [abstract]. Gastrointest Endosc 2002; 55: AB88.
- 8. Ell C, Remke S, May A, et al. The first prospective controlled trial comparing wireless capsule endo-scopy with push enteroscopy in chronic gastro-intestinal bleeding. Endoscopy 2002; 34; 685-689.
- 9. Lewis B, Swain P. Capsule endoscopy in the evalu-ation of patients with suspected small intestinal bleeding: results of a pilot study. Gastrointest Endosc 2002; 56: 349-353.
- 10. Zuckerman R, Prakash C, Askin P, et al. AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 2000; 118: 201-221.
- 11. Costamagna G, Shah A, Riccioni M, et al. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Gastroenterology 2002; 123: 999-1005.
- 12. Jonnalagadda S, Prakash C. Intestinal strictures can impede wireless capsule endoscopy. Gastrointest Endosc 2003; 57: 418-420.
- 13. Eliakim R, Fisher D, Suissa A, et al. Wireless capsule video endoscopy (CE) is a superior diagnostic tool compared with barium follow through (B) and entero-CT (ECT) in patients with suspected Crohn's disease [abstract]. Gastroenterology 2002; 122: A-329.
Abstract
Objectives: To determine the utility of capsule endoscopy in patients referred for investigation of suspected disease of the small intestine.
Design and setting: Single centre, prospective, cohort study from 4 July 2001 to 8 September 2002.
Patients: Sixty consecutive patients who underwent capsule endoscopy for investigation of suspected disease of the small intestine.
Main outcome measures: Abnormal findings at capsule endoscopy.
Results: Examination of the entire small bowel was achieved in 46/60 patients (77%). Thirty-two of 47 patients (68%) referred with obscure gastrointestinal bleeding had positive findings. Seven of nine patients (78%) referred for investigation of suspected Crohn's disease had small bowel erosions or ulcers consistent with Crohn's disease. The capsule was not passed in one patient.
Conclusion: Capsule endoscopy is a novel, minimally invasive and useful tool for the investigation of the small intestine.