




We recently reported that Sydney may be an area of mild iodine deficiency. This hypothesis was based on measurement, in 261 adults, of urine iodine concentration,1 which is accepted as an indicator of iodine status by the World Health Organization (WHO).2 However, we had no outcome data to confirm whether the iodine deficiency we observed was associated with any adverse consequences in this population.
The most important consequence of iodine deficiency is its effect on neurophysiological development, both in utero and in the newborn, and it is now thought to impair brain development indirectly by producing hypothyroidism in both mother and fetus.3 WHO recommends other biological indicators, apart from urine iodine concentration, for determining the severity of iodine deficiency in a population at risk.2 One is the proportion of newborns with whole-blood thyroid-stimulating hormone (TSH) concentrations over 5 mIU/L. (In an iodine-replete population less than 3% of neonates older than 72 hours have a TSH concentration over 5 mIU/L.) Thyroid function in the newborn should reflect fetal thyroid function — if iodine deficiency during pregnancy impairs fetal thyroid function, this should result in higher TSH concentrations in the newborn.
To further investigate our hypothesis of iodine deficiency in northern Sydney, we assessed newborn TSH concentrations, which are assayed as part of a routine neonatal screening program.4 Here, we present data on TSH values in whole blood of a large sample of infants born at RNSH, and, for a small subset of neonates, examine the correlation between concentrations of maternal urinary iodine and neonatal TSH.
All babies in New South Wales have a heel-prick blood sample collected at least 48 hours after birth, usually on Day 3 (the birth date is Day 0), as part of the routine newborn screening program.4 WHO criteria stipulate that samples for TSH measurement should be collected 72 hours after birth5 (to avoid the physiological rise in TSH concentration which occurs immediately after birth). For our study, "Day 3" was the preferred time for sampling, but babies born in the morning may have had samples collected before 72 hours of age.
The heel-prick samples are sent to the central NSW Newborn Screening Laboratory. TSH is measured by dissociation enhanced fluoroimmunoassay (DELFIA) performed on an AutoDELFIA analyser (Wallac/Perkin Elmer Life Sciences, Turku, Finland). Samples with levels > 15 mIU/L are reassayed in triplicate; otherwise assays are performed singly. The between-assay coefficient of variation at a TSH concentration of 15 mIU/L is 6.9%, and at a TSH concentration of 59 mIU/L is 6.5%. The TSH assay can detect levels as low as < 2 mIU/L, defined as 2 SD above the mean of the lowest standard measurement.
To determine the effect on TSH values of the age of the neonate when the heel-prick sample was collected, we analysed TSH values in the subset of 84 infants in relation to (i) time of birth, and (ii) whether the infant was born before or after midday, which would influence whether the Day 3 heel-prick blood sample (which was mostly taken late in the morning) was collected after or before 72 hours of birth.
Iodine determination was performed with a Varian UltraMass inductively coupled plasma mass spectrometer with an SPS-5 autosampler (Varian Inc, Palo Alto, Calif, USA) as described previously.1 Urine creatinine levels were measured and the urine : creatinine ratio calculated as described previously.1
Anonymous TSH values were obtained from two groups of neonates born at RNSH between August 1998 and April 1999 (n = 1317) and between 1 March and 31 December 2000 (n = 1457) to ensure that the results were reproducible. One baby from the initial group had a blood TSH measurement of 319 mIU/L and was later shown to have permanent primary congenital hypothyroidism. This infant was excluded, leaving 1316 in the first group.
TSH values were also obtained for 84 identified babies whose mothers had been seen at RNSH between September 1998 and August 1999, most often because of gestational diabetes. None of these women had an elevated TSH concentration. Their urinary iodine level had been measured at least once during pregnancy. (If more than one sample was collected, the first was used, apart from the one exception discussed below.) This group included 64 pregnant women from our initial report,1 plus an additional 20 pregnant women who had urine samples collected between May and August 1999. To be included in the series, a complete dataset had to be available and the heel-prick sample for measurement of neonatal TSH concentration had to have been collected on Day 3 or later.
The mean age of these mothers was 32 (SD, 5) years, and their urine samples for measurement of iodine concentration were collected at a mean of 10 (SD, 7) weeks before delivery. Their infants were born at a mean of 39.1 (SD, 1.6) weeks' gestation. Neonatal heel-prick samples were collected on Day 3.1 (SD, 0.4) of life. Seventy-seven blood samples for TSH measurement were collected on Day 3, five on Day 4 and two on Day 5. No mother had received iodine supplementation.
One woman with uncontrolled diabetes insipidus had a low urine iodine value. The diabetes insipidus was treated and she received dietary advice about iodine-containing foods. A repeat urine sample was collected after stabilisation 12 weeks before delivery, and the result used in our analysis.
We used SPSS for the statistical analyses.6 TSH values are not normally distributed and therefore are reported as medians with interquartile ranges. The Mann–Whitney U test was used to test for differences in the median levels of TSH between groups. Pearson's correlation coefficient (r) was used to measure the association between the natural log of TSH and other continuous variables. χ2 tests were used to test for differences between proportions.
In the two large population samples of 1316 and 1457 neonates, 8.1% (95% CI, 6.6%–9.5%) and 5.4% (95% CI, 4.3%–6.6%), respectively, had neonatal whole-blood TSH values > 5 mIU/L. Thus, the second sample confirmed the results of the first analysis.
The median TSH value of the 1316 neonates was similar to that of the 84 infants whose mothers had had their urinary iodine concentration measured (1.87 mIU/L v 1.77 mIU/L; P = 0.71) (Box 1), and the proportion of infants in each group with TSH values > 5 mIU/L was also similar (8.1% v 10.7%; P = 0.39).
In the 84 identified neonates, time of birth was not associated with the TSH value (r = 0.002, P = 0.99), and infants born before midday were just as likely to have a TSH value > 5 mIU/L as infants born after midday (Box 2).
The median urine iodine concentration of the 84 mothers was 109 µg/L (65–168 µg/L), and 11.9% (95% CI, 5.0%–18.8%) of the women had a urine iodine concentration < 50 µg/L. Based on WHO criteria for adequate urine iodine concentrations in populations (median value, > 100 µg/L, and < 20% of the population with concentrations < 50 µg/L),2 this subgroup of women is not iodine deficient. However, as iodine requirements are increased in pregnancy, more demanding criteria and a higher urine iodine content could be applied, and these women considered as having borderline mild iodine deficiency.
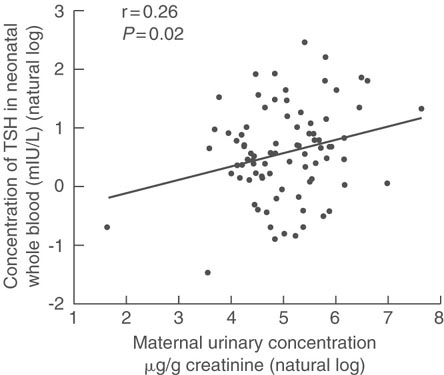
There was a positive correlation between the natural log of neonatal whole blood TSH concentration in mIU/L and the natural log of maternal urine iodine concentration expressed as µg/g creatinine (r = 0.26; P = 0.02) (Box 3). There was a similar correlation between the natural log of neonatal whole-blood TSH concentration in mIU/L and the natural log of iodine concentration in urine in µg/L, but this was not statistically significant (r = 0.21; P = 0.05). Furthermore, no mothers with a low urinary iodine concentration (< 50 µg/L) had an infant with a neonatal TSH measurement > 5 mIU/L.
Our results support the hypothesis that northern Sydney is an area of mild iodine deficiency, with 8.1% and 5.4% of the two large population samples of neonates having TSH values > 5 mIU/L (WHO population prevalence range of neonatal TSH values for classification as mild iodine deficiency, 3%–19.9%).2,5
However, this conclusion should be regarded with some caution. Firstly, the time of sample collection could have influenced the concentration of TSH. In the 84 identified infants, samples for TSH measurement were collected on Day 3, which may have been before 72 hours of life. However, we were unable to find a relationship between TSH concentration and time of birth. In those samples more likely to have been collected within 72 hours of birth, both the TSH values and the proportion of neonates with TSH concentrations > 5 mIU/L were slightly higher, but not significantly so, than in samples more likely to have been collected after 72 hours. A higher TSH level would be anticipated in the samples collected before 72 hours after birth. That the proportion of TSH values > 5 mIU/L in samples more likely to have been collected after 72 hours was still high suggests that early measurement does not fully account for the high proportion of elevated TSH values. A formal study with appropriately timed TSH sampling is required to provide a definitive answer to this question.
Another reason for caution is that the WHO criteria for iodine status do not consider the methods used to assay TSH. Data from the newborn screening quality assurance program of the Centers for Disease Control and Prevention show that different assay methods may produce different results, with variations of up to 15% at a target TSH value of 25 mIU/L among eight methods.7
The vital question "Does the borderline mild iodine deficiency found in the pregnant women account for the high proportion of infants with an elevated TSH?" cannot be answered from the data we present. Moreover, our study raises several other questions and issues. If iodine deficiency is responsible for the elevated neonatal TSH, why is the relationship between maternal urine iodine concentration and neonatal TSH concentration positive? If iodine deficiency were responsible for the higher TSH values, the expected relationship should be negative. A similar lack of the expected relationship between maternal urine iodine and neonatal TSH concentrations has recently also been found in another study.8
Many studies demonstrate the benefit of having an iodine-replete population before pregnancy.9 Iodine deficiency is the leading preventable cause of intellectual impairment.5 Maternal iodine supplementation in populations with high levels of endemic cretinism results in a reduced incidence of cretinism, without significant adverse effects.10 In populations with less severe iodine deficiency without cretinism, the benefit of iodine supplementation is not as rigorously established, although evidence from a meta-analysis of studies suggests that, with iodine supplementation, an improvement in neuropsychological functioning occurs in clinically euthyroid infants from areas with endemic goitre.11 It has been argued that cretinism is merely one end of a continuous spectrum of neuropsychological impairment induced by iodine deficiency, rather than there being a threshold above which cretinism or lesser impairment in neuropsychological development does not occur.12
Iodine deficiency impairs brain development through hypothyroidism. Pop et al have shown that the infants born to mothers who had free thyroxine concentrations below the 10th percentile before week 13 of gestation had impaired neuropsychological development at 10 months and two years.13,14 In the first 12 weeks of fetal life, before fetal thyroid development the fetus depends solely on maternal transfer of thyroxine. The work of Pop et al13,14 was performed in an iodine-replete area.
A formal study of the iodine status of NSW communities should be undertaken.15 It is of vital importance to determine if mild iodine deficiency in Australia might be contributing to subtle maternal hypothyroidism in the early part of pregnancy, with subsequent limitation of neonatal brain development. For this we need to examine the biological effects of the suspected iodine deficiency and, in particular, the biological effects relevant to pregnancy and both maternal and fetal thyroid function.
Specific questions that need to be explored are:
Is the Australian population (or significant sections of the Australian population) suffering from iodine deficiency? and
Do milder degrees of iodine deficiency not associated with cretinism result in impaired neonatal brain development, with a resulting significant permanent decline in cognitive capacity?
Hypothyroidism early in pregnancy, secondary to iodine deficiency, will only be corrected by strategies that ensure adequate iodine intake before pregnancy.16,17
1: Whole-blood thyroid-stimulating hormone (TSH) values (mIU/L) in a general neonatal population (August 1998 – April 1999) and an identified group of neonates
General neonatal population (n = 1316) |
Identified neonatal group (n = 84) |
Test statistic |
|||||||||
Median (interquartile range) TSH concentration (mIU/L) |
1.87 (1.09–3.11) |
1.77 (1.15–2.74) |
Z = 0.37 |
||||||||
Number of neonates (percentage and 95% CI) with TSH values > 5 mIU/L |
106 (8.1%; 6.6%–9.5%) |
9 (10.7%; 4.1%–17.3%) |
χ2 = 0.74 |
||||||||
2: Whole-blood thyroid-stimulating hormone (TSH) values (mIU/L) in the identified group of 84 neonates, according to whether the heel-prick sample was likely to have been collected before or after 72 hours after birth*
Blood sample taken before 72 hours after birth (n = 36) |
Blood sample taken after 72 hours after birth (n = 48) |
Test statistic |
|||||||||||||
Median (interquartile range) TSH concentration (mIU/L) |
1.92 (1.28–3.82) |
1.76 (1.04–2.57) |
Z = 0.69 |
||||||||||||
Number of neonates (percentage and 95% CI) with TSH values > 5 mIU/L |
6 (16.7%; 6.4%–32.8%) |
3 (6.3%; 1.3%–17.2%) |
χ2 = 2.33 |
||||||||||||
*Time of birth (after or before midday) influenced whether the Day 3 heel-prick blood sample (which was mostly taken late in the morning) was collected before or after 72 hours after birth. |
|||||||||||||||
Received 22 March 2001, accepted 20 December 2001
- Aidan McElduff1
- Patrick McElduff4
- Jenny E Gunton2
- Graham Hams3
- Veronica Wiley5
- Bridget M Wilcken6
- 1 Department of Endocrinology, Royal North Shore Hospital, St Leonards, NSW.
- 2 Evidence for Population Health Unit, University of Manchester, Manchester, UK.
- 3 The Children's Hospital at Westmead, Westmead, NSW.
None declared.
- 1. Gunton JE, Hams G, Fiegert M, McElduff A. Iodine deficiency in ambulatory subjects in a Sydney teaching hospital: is Australia truly iodine replete? Med J Aust 1999; 171: 467-470. <eMJA full text>
- 2. World Health Organization. Indicators for assessing iodine deficiency disorders and their control through salt iodization. WHO/NUT/94.6. Geneva: WHO, 1994.
- 3. Hetzel BS. Iodine and neuropsychological development. J Nutr 2000; 130: 493S-495S.
- 4. Wilcken B. Screening In the neonate. In: Trent RJ, editor. Handbook of prenatal diagnosis. Cambridge: Cambridge University Press, 1994: 248-269.
- 5. World Health Organization. Progress towards the elimination of iodine deficiency disorders (IDD). WHO/NUT/99.4. Geneva: WHO, 1999.
- 6. SPSS [computer program], version 9. Chicago, Ill: SPSS Inc, 1999.
- 7. Centers for Disease Control and Prevention Newborn Screening Quality Assurance Program. Atlanta, Ga: CDC, 2000: 17: 4.
- 8. Nohr SB, Laurberg P. Opposite variations in maternal and neonatal thyroid function induced by iodine supplementation during pregnancy. J Clin Endocrinol Metab 2000; 85: 623-627.
- 9. Delange F, Lecomte P. Iodine supplementation benefits outweigh risks. Drug Safety 2000; 22: 89-95.
- 10. Mahomed K, Gulmezoglu AM. Maternal iodine supplements in areas of deficiency (Cochrane Review). In: The Cochrane Library, 2000; Issue 3. Oxford: Update Software.
- 11. Bleichrodt N, Born MP. A metaanalysis of research on iodine and its relationship to cognitive development. In: Stanbury JB, editor. The damaged brain of iodine deficiency. Elmsford, NY: Cognizant Communication Corp 1994; 195-200.
- 12. Boyages S. The damaged brain of iodine deficiency: evidence for a continuum of effect on the population at risk. In: Stanbury JB, editor. The damaged brain of iodine deficiency. Elmsford, NY: Cognizant Communication Corp, 1994: 251-258.
- 13. Pop VJ, Kuijpens JL, van Baar AL, et al. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin Endocrinol (Oxf) 1999; 50: 149-155.
- 14. Pop VJ, Brouwers EP, van Baar AL, et al. Maternal thyroid function during early pregnancy and neurodevelopment of the offspring. Endo 2000. Abstract 163. Available at: http://www.abstracts-on-line.com/abstracts/endo/ (accessed March 2002).
- 15. Boyages SC, Guttikonda K. Iodine status of Australia: look before we leap! Med J Aust 2000; 172: 348.
- 16. Delange F, de Benoist B, Pretell E, Dunn JT. Iodine deficiency in the world: Where do we stand at the turn of the century? Thyroid 2001; 11: 437-447.
- 17. Glinoer D. Pregnancy and iodine. Thyroid 2001; 11: 471-481.
Abstract
Objective: To determine whether thyroid-stimulating hormone (TSH) concentrations in a large sample of neonates meet World Health Organization criteria for an iodine-replete population (< 3% of neonates with whole-blood TSH concentrations > 5 mIU/L), and, in a small subset of neonates, to examine the correlation between maternal urinary iodine and neonatal TSH concentrations.
Design: Cross-sectional study of neonatal whole-blood TSH values obtained as part of a routine newborn screening program.
Setting: Royal North Shore Hospital (RNSH) in northern Sydney.
Participants: Two anonymous samples of neonates born at RNSH (1316 infants born between August 1998 and April 1999 and 1457 infants born between 1 March and 31 December 2000); and 84 infants whose mothers had attended RNSH between September 1998 and August 1999 and supplied a urine sample for iodine measurement.
Main outcome measures: Iodine status of neonates (proportion with whole-blood TSH values > 5 mIU/L), and urine iodine concentrations of pregnant women.
Results: In the two large population samples of neonates, 8.1% (95% CI, 6.6%–9.5%) and 5.4% (95% CI, 4.3%–6.6%), respectively, had whole-blood TSH values > 5 mIU/L (prevalence range for mild thyroid deficiency, 3%–19%). Comparing the TSH values of the 1316 anonymous infants and the 84 identified infants showed no difference between the proportions with TSH values > 5 mIU/L (8.1% v 10.7%, respectively; P = 0.39). Urine iodine concentrations in the 84 pregnant women indicated borderline mild iodine deficiency. TSH values in their 84 infants were positively correlated with maternal urine iodine concentrations.
Conclusions: Our results suggest that the population of northern Sydney may have mild iodine deficiency. However, the expected relationship between maternal urine iodine levels and neonatal TSH concentrations was not found.