




The known Hot water immersion has been shown to be effective for relieving the pain of some jellyfish stings, including blue bottle stings.
The new In the emergency department, hot water immersion was no more effective than icepacks for relieving the pain of major box jellyfish (Chironex fleckeri) stings.
The implications Protocols recommending icepacks for reducing the pain of major box jellyfish stings should not be changed.
The most appropriate treatment of jellyfish stings is controversial. Although hot water immersion is effective and safe for blue bottle (Physalia spp.) stings,1 the evidence is less clear for other types of jellyfish.2 Hot water immersion has been used to treat some box jellyfish (Cubozoa) stings,3 but icepacks remain the standard approach for treating the pain caused by the major box jellyfish, Chironex fleckeri.4,5
C. fleckeri stings are a problem in northern Australia, and severe stings can result in life-threatening envenoming in children. A more common problem is pain, which in more severe cases can persist for several hours and requires parenteral opioid analgesia.4,6 Current protocols in the Northern Territory recommend that, after vinegar has been applied and life-threatening effects have been treated, pain should initially be relieved by applying ice; if this is ineffective, oral or parenteral analgesia can be provided, depending on the severity of the pain.4,6 The effectiveness of hot water immersion for treating the pain of C. fleckeri stings has not been investigated.
Cubozoan venoms are heat-labile, and C. fleckeri venom is inactivated when briefly exposed to temperatures above 43°C.7 Hot water immersion should therefore be as effective for treating C. fleckeri stings as it is for the stings of other jellyfish.1-3,8 If this were the case, it would allow much more rapid treatment and reduce the need for parenteral analgesia (which increases length of stay in the emergency department). A clinical trial of hot water immersion for blue bottle stings found that the technique was safe; as patients were not exposed to temperatures above 46°C, none suffered burns or other adverse effects.1 However, hot water immersion is unlikely to prevent further envenoming from undischarged nematocysts remaining on the skin after a Chironex sting. Applying vinegar is believed to be effective in inactivating undischarged nematocysts, and is preferred to ice or hot water for this purpose.
The aim of our study was to investigate the effectiveness of hot water immersion in the emergency department for relieving the pain of C. fleckeri stings.
Methods
Study design
We undertook an open label, randomised controlled trial that compared hot water immersion (45°C; active treatment) with the application of icepacks (current standard therapy) for treating the pain of C. fleckeri stings in an emergency department in northern Australia.
Patients
Patients who presented with suspected C. fleckeri stings to Royal Darwin Hospital during September 2005 – October 2008 were eligible for the study. They were included if they had been stung within the past 4 hours and the clinical findings were consistent with a C. fleckeri sting (typical local pain; linear red, raised lesions). Children under 8 years of age were excluded because the primary tool for measuring pain, the visual analogue scale (VAS), is not validated for this age group. Patients with severe envenoming that necessitated resuscitation or antivenom, with a sting clinically consistent with Irukandji syndrome and not with a C. fleckeri sting, with stings to the eyes, or with baseline hypotension (blood pressure below 90 mmHg) were also excluded.
Treatment protocol
Patients were assessed and vinegar applied to all sting sites if this had not already been done. Patients meeting the inclusion criteria were then invited to participate, and their consent (or that of their parents or guardians) obtained. A baseline physical examination was undertaken and patients were asked to score their pain on the VAS. Electrocardiography was performed and an intravenous cannula inserted. Patients were then randomised to receive either hot water immersion or icepacks; treatment was randomised by computer in variably sized blocks of 4 or 6 (eg, AABB, ABAB, or ABABAB, AABBAB), according to which a note marked either with “Hot water immersion” or “Icepacks” was placed into sequentially numbered envelopes.
Patients randomised to receiving icepacks were placed in a normal acute care bed, where icepacks were applied to sting sites for 30 minutes (as long as could be tolerated by patients). Patients randomised to receiving hot water immersion were moved to a bath in the emergency department, filled with water that had passed through a thermostatic mixing valve set to 45°C, and the sting area was immersed for 30 minutes. The patient was supervised in this area at all times. For smaller limb or distal stings, a bucket was used instead of the bath, regularly re-filled to maintain its temperature.
During the treatment phase, VAS scores were collected at 10, 20 and 30 minutes, and blood pressure and heart rate were measured at 30 minutes. After completion of treatment, patients were offered the option to change to the other treatment if pain persisted, or were further observed for 30 minutes. A VAS score was again recorded 60 minutes after the beginning of treatment. If pain persisted after 60 minutes, treatment for a further 30 minutes was offered. Patients were then observed and treated according to the normal box jellyfish sting protocol. On discharge from the emergency department (either home or to an inpatient unit), a final VAS score was recorded, and the time of discharge recorded on the datasheet.
Data collection
Demographic information, details of the sting (site, time, conditions, activity), other clinical effects (radiating pain, systemic effects), standard observations (blood pressure, heart rate), and any treatments (analgesia) and length of stay (LOS) in the emergency department were recorded. The Northern Territory Jellyfish Sting Datasheet4,6 was used for most data collection, and a second datasheet was used for recording VAS and other serial data.
Data analysis
The primary outcome was pain severity (as assessed with the VAS) 30 minutes after commencing treatment. A clinically significant change was defined according to the recommendations of Bird and Dickson:9 for an initial VAS in the range 0–33 mm, the clinically significant change is 16 mm; for 34–67 mm, 33 mm; and for 67–100 mm, 48 mm. Secondary outcomes were the proportion of patients who chose to cross to the alternative treatment; the need for repeat treatment for recurrent or ongoing pain; use of opioid analgesia; LOS in the emergency department; development of regional or radiating pain; frequency with which systemic features of stings developed; proportion of patients with papular urticaria when followed up by telephone 7–10 days after discharge.
Our sample size calculation was based on an earlier study of Physalia stings in which the proportion of patients who were pain-free after hot water immersion increased from 33% to 80%.1 To detect whether hot water achieved the same change (α = 0.05; 80% power), 20 patients were needed for each arm of the trial (40 patients in total). One author (GKI) collected the VAS data, extracted the data, and checked outcomes while blinded to treatment. Data analysis was undertaken after the dataset had been finalised.
Medians, ranges and interquartile ranges (IQRs) were calculated for all continuous variables, and 95% confidence intervals (CIs) for proportions. The primary outcome was assessed by intention to treat with the Fisher exact test. Secondary outcomes were analysed with the appropriate statistical tests for their data distribution. For all outcomes, P < 0.05 was deemed statistically significant. All analyses were conducted in Prism 6.03 for Windows (GraphPad Software).
Ethics approval
The study was approved by the Human Research Ethics Committee of the Northern Territory Department of Health and Community Services and Menzies School of Health Research (reference, 05/42). All patients provided written informed consent for the study.
Results
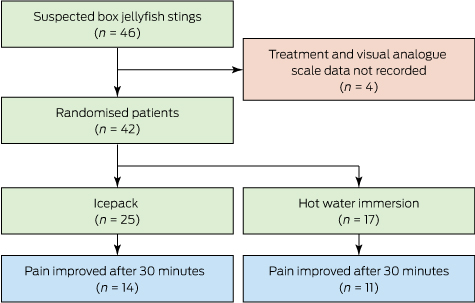
Forty-six patients were recruited, but pain scores and treatment allocation for four people were not recorded. Of the 42 included patients (median age, 19 years; IQR, 13–27 years; 26 were male), 25 were allocated to icepacks and 17 to hot water immersion (Box 1). Twenty patients (48%) had distal limb stings and 14 (33%) developed systemic effects. The demographic, baseline VAS and systemic effects data were similar for the two groups (Box 2). All patients were discharged home from the emergency department, by which time the pain had resolved for 40 of the 42 patients. The median LOS in the emergency department for the 42 patients was 1.8 h (range, 0.5–6.0 h; IQR, 1.1–2.2 h).
Primary outcome
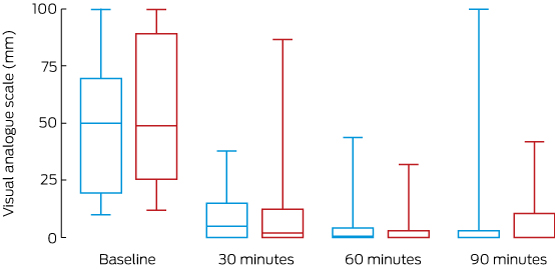
Thirty minutes after treatment commenced, the pain of 14 of 25 of patients (56%) treated with icepacks and of 17 patients (65%) treated with hot water had clinically improved (absolute difference, hot water v icepacks, 9%; 95% CI, –22% to 39%; P = 0.75; Box 3). There was no statistically significant difference between the two treatment arms in the changes in absolute VAS over 90 minutes (Box 4).
Secondary outcomes
One patient in the icepack arm crossed over to hot water immersion; two patients in each arm received intravenous opioid analgesia. The median emergency department LOS for patients treated with icepacks was 1.6 h (IQR, 1.0–1.8 h), for those treated with hot water immersion it was 2.1 h (IQR, 1.6–2.8 h; P = 0.07). No patients re-presented with recurrent pain or developed hypotension. Of seven patients we could follow up, five had developed delayed hypersensitivity rashes.
Discussion
We found that hot water immersion was no better than icepacks for treating the acute pain of C. fleckeri stings. The pain of more than half the patients in each treatment group had decreased after 30 minutes; almost all were discharged from hospital pain-free. There were no severe stings, consistent with severe envenoming being rare.4 Hot water immersion increased the LOS in the emergency department by about 30 minutes, probably because of the practicalities involved in this treatment. There were no differences between groups in the need for opioid analgesia, treatment of recurrent pain, or systemic effects.
The finding that hot water was no more effective than icepacks was unexpected in light of its highly beneficial effect for blue bottle (Physalia) stings.1 Interestingly, the reduction in pain achieved by icepacks in our study (56% at 30 min) was greater than for Physalia stings (33% at 20 min), but the effect of hot water immersion was lower (65% v 87%). There are several potential explanations for the differences, including differing sensitivities of jellyfish venoms to heat. We cannot assume that the effects of treating pain caused by one jellyfish group can be extrapolated to other jellyfish.
Hot water and icepacks were equally effective in our study, possibly because treatment was delayed until the patient reached the emergency department. In the study of Physalia stings,1 hot water immersion was initiated on the beach, often within minutes of the patient being stung, when heat is more likely to be effective. The delay in treatment in our study allowed more time for venom to be absorbed. The effect of heat was therefore more likely to have been symptomatic, rather than providing definitive treatment by inactivating venom. Hot water immersion should be further investigated in a pre-hospital study.
Measurement of pain can be problematic, and a number of tools have been developed. The VAS is one of the most commonly used, including in earlier studies of blue bottle stings1 and red-back spider bites.10 More recent studies have employed a verbal numerical rating score because it is easier to administer (paper is not required)11 and it is used in clinical practice; management of C. fleckeri stings should now include regular assessment of the pain with the verbal numerical score. Correcting for the baseline pain score is controversial, but it enables comparison of patients with differing severity of subjective pain, and this approach has been applied in three previous studies of painful envenoming syndromes.1,10,11 Responses to treatment in our study were similar when relative (Box 3) and absolute VAS (Box 4) data were analysed.
One limitation of our study is that the diagnosis of C. fleckeri envenoming was made clinically; that is, there was no direct evidence that the jellyfish involved in any particular case was C. fleckeri. Previous studies have found, however, that C. fleckeri is the dominant box jellyfish in Darwin Harbour,4,6 with the only other recorded multi-tentacle stings being minor stings by the Darwin carybdeid (four-tentacled box jellyfish), Gerongia rifkinae.12
A further limitation of the study was the small sample size, the result of our anticipating a larger treatment effect for hot water immersion than for icepacks. A larger study would have been required to detect whether hot water immersion had a smaller beneficial effect than icepacks. As investigations of the effectiveness of analgesia usually require large treatment effects (25–50% difference) for the results to be regarded as clinically significant, a larger study may have found a statistically significant difference between the two treatments that was not clinically significant. Another limitation associated with the small sample sizes was the unequal allocation of patients to the two groups because of the block size and exclusions we applied.
Icepacks are simpler, more practical and potentially safer than hot water immersion for the emergency department treatment of box jellyfish stings in tropical Australia. As hot water immersion achieved no major benefit but increased the emergency department LOS, icepacks are more appropriate and remain the recommended emergency department treatment for reducing the pain of major box jellyfish stings after applying vinegar to the wound.
Box 1 – CONSORT diagram for the study of people with suspected Chironex fleckeri stings presenting to the Royal Darwin Hospital emergency department, September 2005 – October 2008
Box 2 – Demographic characteristics of the patients allocated to treatment with hot water immersion or icepacks, and the clinical effects associated with treatment
|
|
Icepacks |
Hot water immersion |
|||||||||||||
|
|
|||||||||||||||
|
Number of patients |
25 |
17 |
|||||||||||||
|
Sex (males) |
15 (60%) |
11 (65%) |
|||||||||||||
|
Age (years), median (IQR) |
22 (15–30) |
14 (9–23) |
|||||||||||||
|
Sting site: distal limb |
11 (44%) |
9 (53%) |
|||||||||||||
|
Systemic effects |
9 (36%) |
5 (29%) |
|||||||||||||
|
Gastrointestinal (nausea/vomiting) |
5 (20%) |
2 (12%) |
|||||||||||||
|
Respiratory (shortness of breath) |
2 (8%) |
3 (18%) |
|||||||||||||
|
Generalised pain |
2 (8%) |
2 (12%) |
|||||||||||||
|
Baseline visual analogue score, median (IQR) |
50 (20–70) |
49 (26–90) |
|||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Box 3 – Proportional change in visual analogue scale (VAS) score after 30 minutes’ treatment with icepacks or hot water immersion*
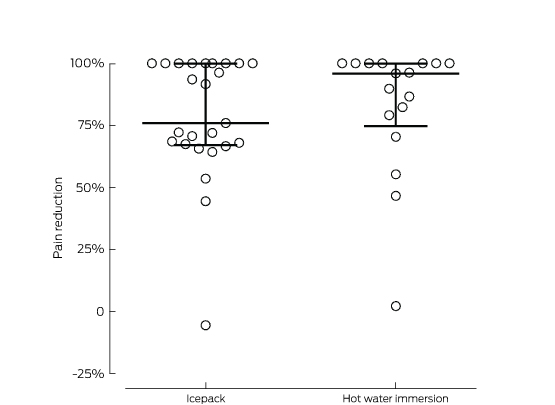
* The lines mark the medians and interquartile ranges for each treatment group. The difference between the median percentage change in VAS (icepack, 76%; hot water immersion, 96%) was not statistically significant (P = 0.46).
Received 22 August 2016, accepted 17 October 2016
- Geoffrey K Isbister1,2
- Didier J Palmer3
- Rebecca L Weir3,4
- Bart J Currie5
- 1 University of Newcastle, Newcastle, NSW
- 2 Calvary Mater Newcastle, Newcastle, NSW
- 3 Royal Darwin Hospital, Darwin, NT
- 4 North East Health Wangaratta, Wangaratta, VIC
- 5 Menzies School of Health, Royal Darwin Hospital, Darwin, NT
Geoff Isbister is supported by a National Health and Medical research Council Senior Research Fellowship (1061041). The study was supported by a Morson Taylor Research Award.
No relevant disclosures.
- 1. Loten C, Stokes B, Worsley D, et al. A randomised controlled trial of hot water (45°C) immersion versus ice packs for pain relief in bluebottle stings. Med J Aust 2006; 184: 329-333. <MJA full text>
- 2. Li L, McGee RG, Isbister G, Webster AC. Interventions for the symptoms and signs resulting from jellyfish stings. Cochrane Database Syst Rev 2013; (12): CD009688.
- 3. Thomas CS, Scott SA, Galanis DJ, Goto RS. Box jellyfish (Carybdea alata) in Waikiki: their influx cycle plus the analgesic effect of hot and cold packs on their stings to swimmers at the beach: a randomized, placebo-controlled, clinical trial. Hawaii Med J 2001; 60: 100-107.
- 4. Currie BJ, Jacups SP. Prospective study of Chironex fleckeri and other box jellyfish stings in the “Top End” of Australia’s Northern Territory. Med J Aust 2005; 183: 631-636. <MJA full text>
- 5. Toxicology and Wilderness Expert Group. Therapeutic guidelines: toxicology and wilderness, version 2. Melbourne: Therapeutic Guidelines, 2012.
- 6. O’Reilly GM, Isbister GK, Lawrie PM, et al. Prospective study of jellyfish stings from tropical Australia, including the major box jellyfish Chironex fleckeri. Med J Aust 2001; 175: 652-655. <MJA full text>
- 7. Carrette TJ, Cullen P, Little M, et al. Temperature effects on box jellyfish venom: a possible treatment for envenomed patients? Med J Aust 2002; 177: 654-655. <MJA full text>
- 8. Nomura JT, Sato RL, Ahern RM, et al. A randomized paired comparison trial of cutaneous treatments for acute jellyfish (Carybdea alata) stings. Am J Emerg Med 2002; 20: 624-626.
- 9. Bird SB, Dickson EW. Clinically significant changes in pain along the visual analog scale. Ann Emerg Med 2001; 38: 639-643.
- 10. Isbister GK, Brown SG, Miller M, et al. A randomised controlled trial of intramuscular vs. intravenous antivenom for latrodectism — the RAVE study. QJM 2008; 101: 557-565.
- 11. Isbister GK, Page CB, Buckley NA, et al. Randomized controlled trial of intravenous antivenom versus placebo for latrodectism: the second Redback Antivenom Evaluation (RAVE-II) study. Ann Emerg Med 2014; 64: 620-628. e2.
- 12. Gershwin L, Alderslade P. A new genus and species of box jellyfish (Cubozoa: Carybdeidae) from tropical Australian waters. The Beagle: Records of the Museums and Art Galleries of the Northern Territory 2005; 21 (Dec): 27-36.
Abstract
Objective: To investigate the effectiveness of hot water immersion for relieving the pain of major box jellyfish (Chironex fleckeri) stings.
Design, interventions: Open label, randomised controlled trial comparing the effects of hot water immersion (45°C) and icepacks.
Setting, participants: 42 patients with suspected C. fleckeri stings treated in the emergency department of the Royal Darwin Hospital during September 2005 – October 2008.
Main outcome measures: The primary outcome was pain severity, assessed with a visual analogue scale (VAS). Secondary outcomes included crossover to the alternative treatment, use of opioid analgesia, emergency department length of stay (LOS), and delayed urticaria.
Results: Of 42 patients (26 males; median age, 19 years; IQR, 13–27 years), 25 were allocated to icepack treatment and 17 to hot water immersion. The demographic and baseline VAS data for the two groups were similar. After 30 minutes of treatment, 11 patients (65%) treated with hot water and 14 (56%) treated with icepacks had clinically improved pain scores (absolute difference, 9%; 95% CI, –22% to 39%; P = 0.75). One patient treated with icepacks crossed over to heat immersion. Two patients in each arm received intravenous opioid analgesia. Median emergency department LOS was 1.6 h (IQR, 1.0–1.8 h) for icepack patients and 2.1 h (IQR, 1.6–2.8 h) for heat immersion patients (P = 0.07). Five of seven patients who were followed up developed delayed urticaria.
Conclusion: Hot water immersion was no more effective than icepacks for reducing the acute pain of box jellyfish stings, but increased emergency department LOS by about 30 minutes.
Trial registration: Australian New Zealand Clinical Trials Registry, ACTRN12605000007639.