




Improving hand hygiene practices in health care has been a major challenge for more than 160 years.1 Despite much evidence that hand hygiene practices are effective in preventing infection and reducing the spread of microbial resistance, the hand-cleaning behaviour of health care workers (HCWs) remains largely unchanged.2 Indeed, in almost all settings where it has been assessed, compliance with hand hygiene practices at appropriate times during the course of patient care has been less than 50%. But should HCWs carry all the blame? How do working conditions affect hand hygiene behaviour? Can behaviour change? If so, how much change in individual behaviour is necessary to reflect change at a group level? Is a major system change sufficient to transform practices? Is hand hygiene behaviour integrated into the theory of ecological perspective3 once change is targeted? What should the targets for improvement be? How far can HCWs be expected to modify their practices? How long will it take to succeed? How can behavioural change be sustained, if and when it is achieved? What does “success” mean in terms of hand hygiene promotion? What are the best indicators of success? How much local success is needed to predict more global achievements?
These are some of the many questions to be kept in mind by all those embarking on hand hygiene promotion. Successful promotion is a crusade, and we should not forget the “first crusader”, Ignaz Semmelweis, who paved the way in 1847.1 Semmelweis’s crusade was long and difficult and, although extremely beneficial to patient safety, it was certainly not rewarding for him, and was even detrimental to his career.4 But attitudes and evidence have changed over the past 162 years. Thankfully, it is now well established that successful hand hygiene promotion does not result from forcing HCWs to plunge their hands into a caustic, chlorinated lime solution before patient contact and accusing them of being murderers if they refuse!
Ample evidence suggests that successful hand hygiene promotion is the result of multimodal strategies involving multiple partners and key players.2 The proposed, tested and validated World Health Organization strategy now used in many hospitals worldwide (Box 1) includes at least five key elements: homogeneous HCW education; performance monitoring and feedback; reminders in the workplace; facilitated access to alcohol-based hand rub (AHR) at the point of patient care; and promotion of a safety culture at all levels.2,5 This strategy has been modelled on previous longstanding experience at the University of Geneva hospitals6,7 before being adopted at single8,9 and multiple institutions10,11 and, importantly, adapted to different cultures for worldwide use in both developed and developing countries.12,13
Clean hands save lives is a good example of a statewide multimodal promotion campaign. The strategy included monitoring of HCWs’ compliance, with performance feedback; using staff “champions” and local leaders; placing reminders in the workplace; engaging patients and their families; and ensuring the availability of AHR at the point of care. This supplement includes four reports that summarise important aspects of the project’s management and present early results relating to structures, processes and outcomes.14-17
System change has been one of the first measurable, successful achievements of the Clean hands save lives campaign. Over a period of less than 6 months, the availability of AHR at the point of care improved markedly, to the point where 70% of all available hospital beds in New South Wales had at least one AHR dispenser nearby. Importantly, such a system change must be sustainable, with a measurable increase in AHR use over time.6,7
System change implies culture change.18,19 Pre- and post-campaign surveys showed that the NSW campaign significantly raised HCWs’ awareness of hand hygiene and improved their perceptions of the need for the campaign and of its ability to help improve their own practices. Most HCWs believed that they could sustain system and behavioural change over time, and some even gained sufficient confidence to remind their peers. Furthermore, a quarter of surveyed patients and hospital visitors said they would be willing to actively participate in hand hygiene promotion by reminding staff about hand hygiene. Thus, the Clean hands save lives campaign clearly initiated a culture change at an organisational6,20 and possibly regional level. It helped to promote positive attitudes and dispel negative perceptions held by staff, patients, and visitors. Whether such a change has been sufficiently embedded in health care organisations at all levels to induce individual and institutional accountability remains to be evaluated in the near future.
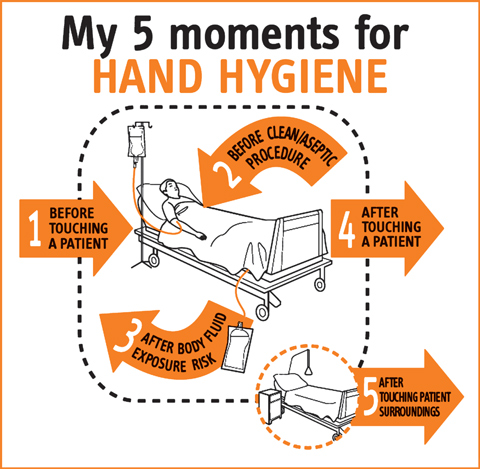
Among the campaign’s process and outcome measures were compliance with hand hygiene practices and monitoring of methicillin-resistant Staphylococcus aureus (MRSA) cross-transmission and infection rates. Overall hand hygiene compliance, monitored before and after patient contact, improved from 47% to an average of 61%, and all categories of HCW except medical staff improved their compliance. As universally reported,2,6,8-13,18-20 compliance after patient contact was markedly better than before patient contact, emphasising the need for further education to improve patient safety. Preventing pathogen transmission to patients relies above all on cleaning hands before touching each patient, before performing clean and aseptic tasks,21,22 after contact with a patient or the patient’s close environment, or after exposure to body fluids. Respecting these recommendations will mostly protect HCWs and patients and prevent environmental contamination (Box 2). Whether the observed improvement in hand hygiene compliance between the pre- and post-campaign periods may have been partly due to a Hawthorne effect is debatable. However, such an effect need not be considered an undesirable outcome if it contributes to positive culture change. Although improvement in hand hygiene practice was paralleled with some measurable reductions in indicators of MRSA infection, the effect of major confounders should be recognised, particularly in the context of statewide surveillance and interventions.
In summary, the Clean hands save lives campaign has achieved remarkable success in NSW health care institutions — system change, culture change and practice improvement, with early signs of an impact on some patient safety indicators. Ensuring the sustainability of the campaign, together with organisational and regional changes to foster accountability at different levels, will be challenging. Further improvement will require HCWs to integrate the “My five moments for hand hygiene” concept (Box 2)22 into their thinking and routine behaviour and thus shift the focus towards greater patient safety. Further development of the concept of staff champions and local leaders to drive compliance improvement among all HCWs, particularly medical staff, is critical.23 Importantly, all health care institutions in NSW need to adopt the Clean hands save lives strategy.
Successful diffusion of innovation and change requires adaptation.2,18,24 Campaign strategists and crusaders need to understand that having the support of management can be extremely helpful in making a campaign more cost-effective. Adaptation of tools and interventions to local needs is critical for universal endorsement, sustainability and long-term success. Combining the efforts and successes of the NSW campaign with the statewide campaign in Victoria10 would be a positive move towards the future roll-out of national action in Australia, and would follow the example of more than 40 campaigning countries worldwide.25,26

- 1. Pittet D, Boyce JM. Hand hygiene and patient care: pursuing the Semmelweis legacy. Lancet Infect Dis 2001; 1: 9-20.
- 2. World Health Organization. WHO guidelines for hand hygiene in health care. First global patient safety challenge: clean care is safer care. Geneva: WHO, 2009. http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf (accessed Sep 2009).
- 3. Pittet D. The Lowbury lecture: behaviour in infection control. J Hosp Infect 2004; 58: 1-13.
- 4. Pittet D. The crusade against puerperal fever. Lancet 2004; 363: 1331-1332.
- 5. World Health Organization. Clean care is safer care. Multimodal Hand Hygiene Improvement Strategy. Implementation toolkit. http://www.who.int/gpsc/5may/tools/en/index.html (accessed Jun 2009).
- 6. Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Infection Control Programme. Lancet 2000; 356: 1307-1312.
- 7. Pittet D, Sax H, Hugonnet S, Harbarth S. Cost implications of successful hand hygiene promotion. Infect Control Hosp Epidemiol 2004; 25: 264-266.
- 8. Johnson PDR, Martin R, Burrell LJ, et al. Efficacy of an alcohol/chlorhexidine hand hygiene program in a hospital with high rates of nosocomial methicillin-resistant Staphylococcus aureus (MRSA) infection. Med J Aust 2005; 183: 509-514. <MJA full text>
- 9. Harbarth S, Pittet D, Grady L, et al. Interventional study to evaluate the impact of an alcohol-based hand gel in improving hand hygiene compliance. Pediatr Infect Dis J 2002; 21: 489-495.
- 10. Grayson ML, Jarvie LJ, Martin R, et al. Significant reductions in methicillin-resistant Staphylococcus aureus bacteraemia and clinical isolates associated with a multisite, hand hygiene culture-change program and subsequent successful statewide roll-out. Med J Aust 2008; 188: 633-640. <MJA full text>
- 11. National Patient Safety Agency. Cleanyourhands campaign. http://www.npsa.nhs.uk/cleanyourhands (accessed Jun 2009).
- 12. Allegranzi B, Pittet D. Preventing infections acquired during health-care delivery. Lancet 2008; 372: 1719-1720.
- 13. Ahmed QA, Memish ZA, Allegranzi B, Pittet D; WHO Global Patient Safety Challenge. Muslim health-care workers and alcohol-based handrubs. Lancet 2006; 367: 1025-1027.
- 14. Pantle AC, Fitzpatrick KR, McLaws ML, Hughes CF. A statewide approach to systematising hand hygiene behaviour in hospitals: Clean hands save lives, Part I. Med J Aust 2009; 191 (8 Suppl): S8-S12. <MJA full text>
- 15. Fitzpatrick KR, Pantle AC, McLaws ML, Hughes CF. Culture change for hand hygiene: Clean hands save lives, Part II. Med J Aust 2009; 191 (8 Suppl): S13-S17. <MJA full text>
- 16. McLaws ML, Pantle AC, Fitzpatrick KR, Hughes CF. Improvements in hand hygiene across New South Wales public hospitals: Clean hands save lives, Part III. Med J Aust 2009; 191 (8 Suppl): S18-S25. <MJA full text>
- 17. McLaws ML, Pantle AC, Fitzpatrick KR, Hughes CF. More than hand hygiene is needed to affect methicillin-resistant Staphylococcus aureus clinical indicator rates: Clean hands save lives, Part IV. Med J Aust 2009; 191 (8 Suppl): S26-S31. <MJA full text>
- 18. Pittet D. The Lowbury lecture: behaviour in infection control. J Hosp Infect 2004; 58: 1-13.
- 19. Whitby M, Pessoa-Silva CL, McLaws ML, et al. Behavioural considerations for hand hygiene practices: the basic building blocks. J Hosp Infect 2007; 65: 1-8.
- 20. Larson EL, Early E, Cloonan P, et al. An organizational climate intervention associated with increased handwashing and decreased nosocomial infections. Behav Med 2000; 26: 14-22.
- 21. Pittet D, Allegranzi B, Sax H, et al. Evidence-based model for hand transmission during patient care and the role of improved practices. Lancet Infect Dis 2006; 6: 641-652.
- 22. Sax H, Allegranzi B, Uçkay I, et al. “My five moments for hand hygiene”: a user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect 2007; 67: 9-21.
- 23. Pittet D, Simon A, Hugonnet S, et al. Hand hygiene among physicians: performance, beliefs, and perceptions. Ann Intern Med 2004; 141: 1-8.
- 24. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: setting a goal and a deadline for improving health care quality. JAMA 2006; 295: 324-327.
- 25. Pittet D, Donaldson L. Clean Care is Safer Care: a worldwide priority. Lancet 2005; 366: 1246-1247.
- 26. Clinical Excellence Commission. Clean hands save lives: final report of the NSW Hand Hygiene Campaign. Sydney: NSW Health, 2007. http://www.cec.health.nsw.gov.au/moreinfo/cleanhands_report.html (accessed Aug 2009).
I wish to thank all members of the Infection Control Programme at the University of Geneva hospitals, in particular Rosemary Sudan, for expert editorial assistance, and members of the World Health Organization’s First Global Patient Safety Challenge core group: John Boyce, Barry Cookson, Nizam Damani, Don Goldmann, Lindsay Grayson, Elaine Larson, Geeta Mehta, Ziad Memish, Hervé Richet, Manfred Rotter, Syed Sattar, Hugo Sax, Wing Hong Seto, Andreas Voss and Andreas Widmer. I would also like to thank William Griffiths, Julie Storr and Orlando Urroz. The WHO takes no responsibility for the information provided or the views expressed in this article.
None identified.